Relying on other people is not a disorder. Humans are interdependent by design — we lean on partners, friends, and family for support, advice, and comfort, and that’s healthy. Dependent Personality Disorder (DPD) is something more specific and more impairing: a pervasive, excessive need to be taken care of that produces submissive, clinging behavior and intense fear of separation. The reliance crosses from preference into a genuine difficulty functioning independently — struggling to make ordinary decisions without reassurance, avoiding disagreement to keep others close, and feeling helpless or panicked at the prospect of being alone.
This free Dependent Personality Disorder Test screens for the traits of DPD using the DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Instant, private results. It’s a reflection tool, not a diagnosis — only a qualified professional can diagnose a personality disorder, and the line between strong attachment and a clinical disorder is one that requires clinical judgment to draw.
What Is Dependent Personality Disorder?
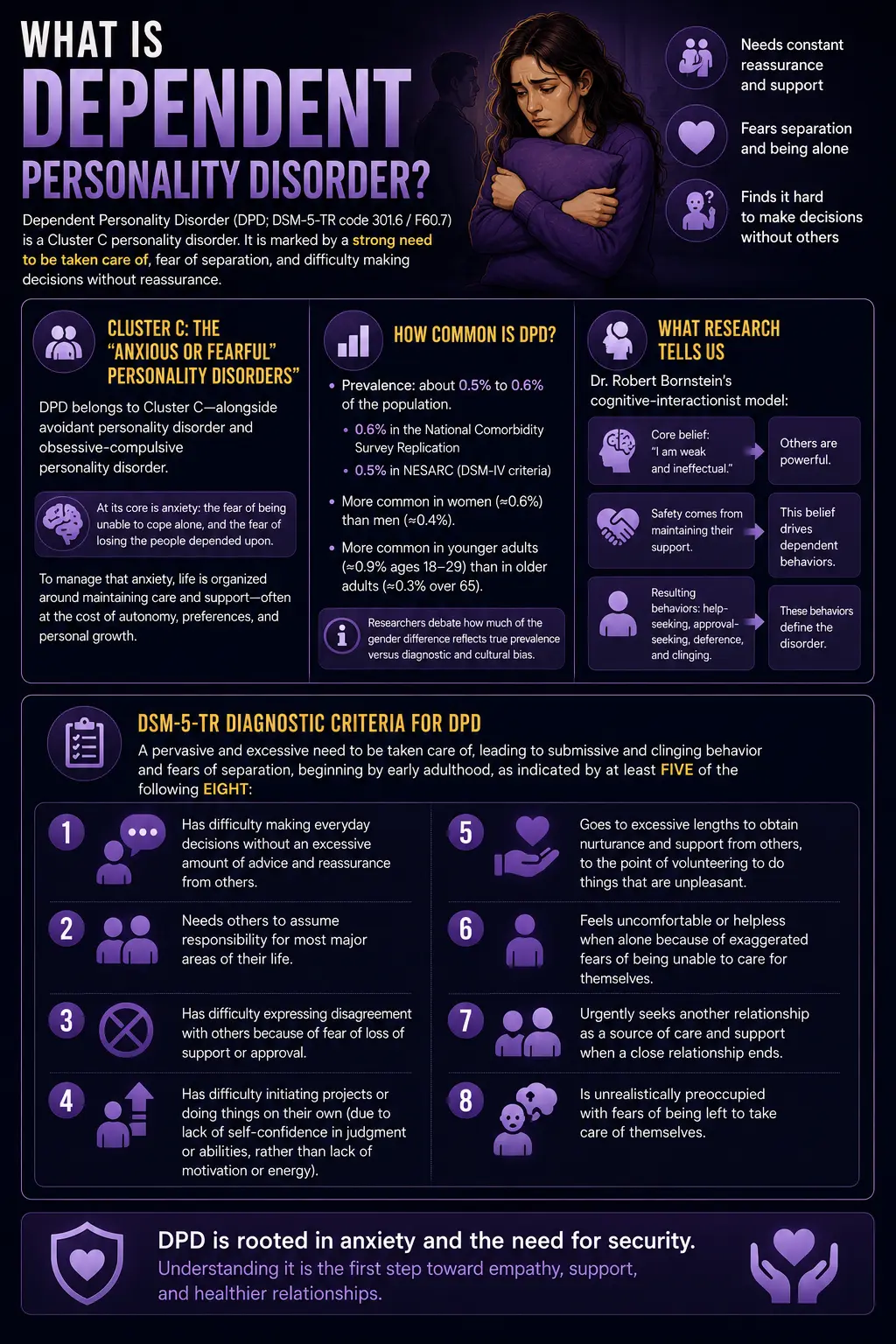
Dependent Personality Disorder (DPD; DSM-5-TR code 301.6 / F60.7) is a Cluster C personality disorder defined by a pervasive and excessive need to be taken care of that leads to submissive and clinging behavior and fears of separation, beginning by early adulthood and present across many contexts. People with DPD have great difficulty making everyday decisions without reassurance, tend to let others take responsibility for major areas of their lives, struggle to disagree for fear of losing support, and feel intensely uncomfortable or helpless when alone.
DPD belongs to Cluster C — the “anxious or fearful” personality disorders — alongside avoidant personality disorder and obsessive-compulsive personality disorder. At its core is anxiety: the fear of being unable to cope alone, and the fear of losing the people depended upon. To manage that anxiety, the person organizes their life around maintaining care and support — often at the cost of their own autonomy, preferences, and growth.
DPD is one of the less common personality disorders. Prevalence estimates cluster around 0.5% to 0.6% of the population (the National Comorbidity Survey Replication found 0.6%; NESARC data using DSM-IV criteria found 0.5%), making it among the least prevalent of the ten personality disorders (StatPearls; Merck Manual). It is diagnosed more often in women (around 0.6%) than men (around 0.4%), though researchers debate how much of this reflects true prevalence versus diagnostic and cultural bias — dependency is more socially reinforced and less pathologized in women, which may skew both self-presentation and clinician judgment. DPD is also more common in younger adults (about 0.9% among those aged 18–29) than in older adults (about 0.3% over 65).
The most influential modern researcher on dependency is Dr. Robert Bornstein, whose cognitive-interactionist model frames dependency around a core belief of being weak and ineffectual combined with the perception that others are powerful and that safety comes from maintaining their support. This belief system then drives the behaviors — help-seeking, approval-seeking, deference — that define the disorder.
The full DSM-5-TR criteria require a pervasive and excessive need to be taken care of, leading to submissive and clinging behavior and fears of separation, beginning by early adulthood, as indicated by at least five of the following eight (APA, 2022):
- Has difficulty making everyday decisions without an excessive amount of advice and reassurance from others.
- Needs others to assume responsibility for most major areas of their life.
- Has difficulty expressing disagreement with others because of fear of loss of support or approval.
- Has difficulty initiating projects or doing things on their own (due to lack of self-confidence in judgment or abilities, rather than lack of motivation or energy).
- Goes to excessive lengths to obtain nurturance and support from others, to the point of volunteering to do things that are unpleasant.
- Feels uncomfortable or helpless when alone because of exaggerated fears of being unable to care for themselves.
- Urgently seeks another relationship as a source of care and support when a close relationship ends.
- Is unrealistically preoccupied with fears of being left to take care of themselves.
Signs You Might Have Dependent Personality Disorder
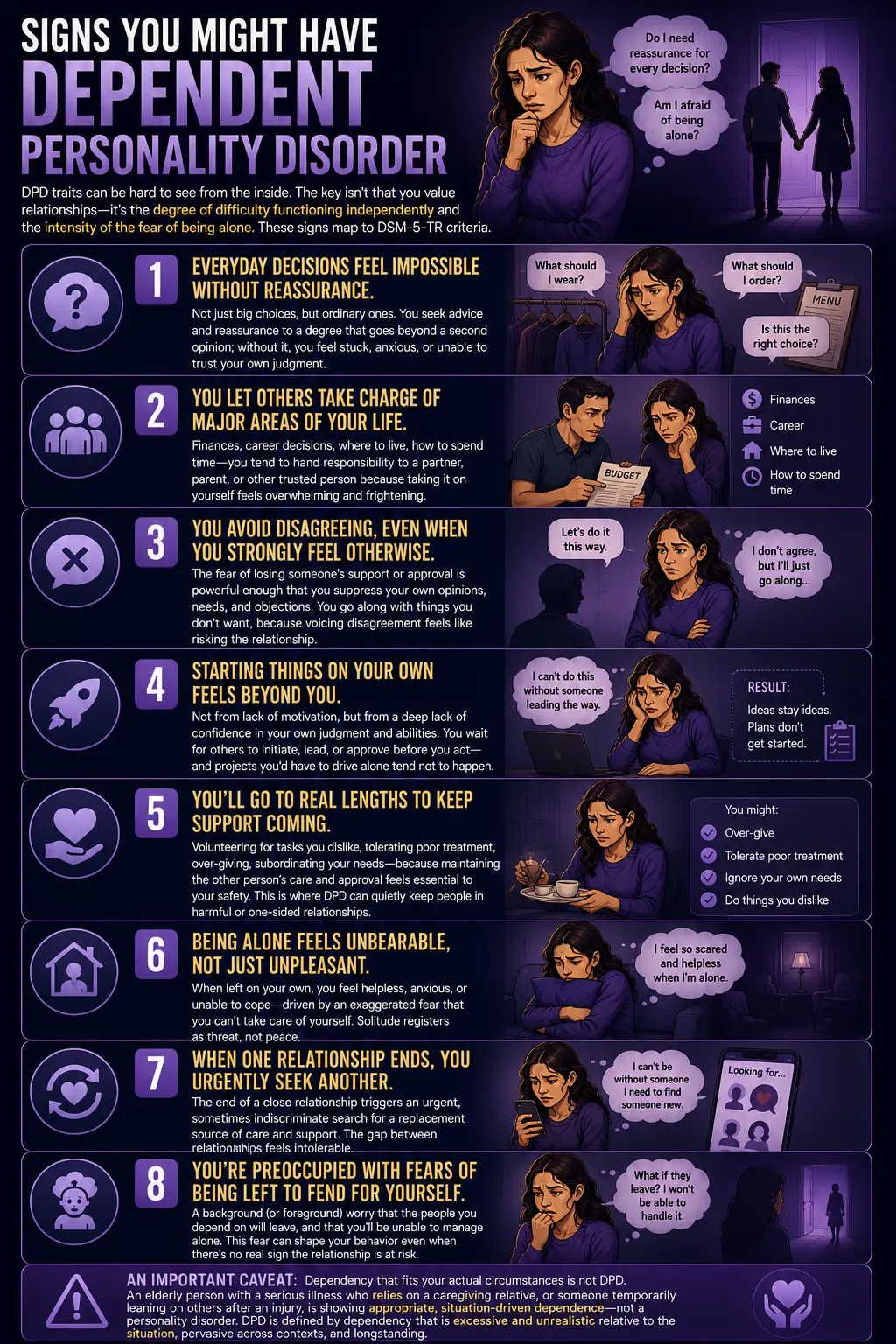
DPD traits can be hard to see from the inside, because the behaviors often feel like love, loyalty, or simply “being a supportive partner.” The distinguishing feature isn’t that you value relationships — it’s the degree of difficulty functioning independently and the intensity of the fear of being alone. These are the signs most consistent with DPD, mapped to the DSM-5-TR criteria.
Everyday decisions feel impossible without reassurance. Not just big choices, but ordinary ones — what to wear, what to order, how to handle a small work task. You seek advice and reassurance to a degree that goes beyond wanting a second opinion; without it, you feel stuck, anxious, or unable to trust your own judgment.
You let others take charge of major areas of your life. Finances, career decisions, where to live, how to spend time — you tend to hand responsibility for these to a partner, parent, or other trusted person, not because you can’t in principle, but because taking it on yourself feels overwhelming and frightening.
You avoid disagreeing, even when you strongly feel otherwise. The fear of losing someone’s support or approval is powerful enough that you suppress your own opinions, needs, and objections. You go along with things you don’t want, because voicing disagreement feels like risking the relationship.
Starting things on your own feels beyond you. Not from lack of motivation, but from a deep lack of confidence in your own judgment and abilities. You wait for others to initiate, lead, or approve before you act — and projects you’d have to drive alone tend not to happen.
You’ll go to real lengths to keep support coming. Volunteering for tasks you dislike, tolerating poor treatment, over-giving, subordinating your needs — because maintaining the other person’s care and approval feels essential to your safety. This is where DPD can quietly keep people in harmful or one-sided relationships.
Being alone feels unbearable, not just unpleasant. When left on your own, you feel helpless, anxious, or unable to cope — driven by an exaggerated fear that you can’t take care of yourself. Solitude registers as threat, not peace.
When one relationship ends, you urgently seek another. The end of a close relationship isn’t just painful; it triggers an urgent, sometimes indiscriminate search for a replacement source of care and support. The gap between relationships feels intolerable.
You’re preoccupied with fears of being left to fend for yourself. A background (or foreground) worry that the people you depend on will leave, and that you’ll be unable to manage alone. This fear can shape your behavior even when there’s no real sign the relationship is at risk.
An important caveat: dependency that fits your actual circumstances is not DPD. An elderly person with a serious illness who relies heavily on a caregiving relative, or someone temporarily leaning on others after an injury, is showing appropriate, situation-driven dependence — not a personality disorder. DPD is defined by dependency that is excessive and unrealistic relative to the situation, pervasive across contexts, and longstanding.
DPD vs Codependency vs Avoidant PD vs BPD
| Feature | Dependent PD | Codependency | Avoidant PD | Borderline PD |
|---|---|---|---|---|
| Core pattern | Excessive need to be taken care of; reliance on others to function | Compulsive caretaking of others, often at own expense | Avoidance of relationships from fear of rejection | Unstable relationships, identity, and emotions; fear of abandonment |
| Direction of dependence | Being cared for — receiving support and direction | Caring for — being needed by someone (often an addicted/impaired partner) | Wants closeness but withdraws to avoid anticipated rejection | Intense push-pull; craves closeness, fears engulfment and abandonment |
| Clinical status | DSM-5-TR personality disorder (301.6) | Not a DSM diagnosis; a widely-used clinical/self-help concept | DSM-5-TR personality disorder (301.82) | DSM-5-TR personality disorder (301.83) |
| Relationship to being alone | Feels helpless; urgently seeks a replacement relationship | May tolerate being alone but feels worthless without someone to help | May prefer some distance despite longing; fears the relationship itself | Abandonment triggers intense emotional crises |
| PsyMed test | This test | Codependency Test | Avoidant PD Test | BPD Test |
Two distinctions matter most. First, DPD vs codependency: these are often confused, but the direction of dependence differs. DPD centers on the need to be taken care of — receiving support, direction, and decisions from others. Codependency (not a formal DSM diagnosis) typically centers on compulsive caretaking of others — deriving identity and worth from being needed, often in relationships with an addicted or impaired partner. A person can have both, but they are distinct patterns.
Second, DPD vs avoidant personality disorder: both are Cluster C and both involve anxiety and low self-confidence, but they respond in opposite directions. The person with avoidant PD withdraws from relationships until they’re certain of uncritical acceptance; the person with DPD actively seeks out and clings to relationships (Merck Manual). One avoids to prevent rejection; the other attaches to prevent abandonment. Interestingly, twin research suggests avoidant and dependent PD share some heritable basis (Gjerde et al., 2012), which fits their overlapping anxious, self-doubting core.
Understanding Your Dependent Personality Disorder Test Score
A note before your result: this score reflects how strongly your answers align with dependent traits — it’s a starting point for reflection, not a diagnosis. Many people have some dependent traits without having the disorder, and healthy interdependence is not being measured against you here. Only a qualified professional can diagnose DPD, which requires a pervasive, longstanding pattern that causes real impairment.
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Minimal — Few Dependent Traits | Few dependent traits indicated. Healthy reliance on others may be present without the excessive dependency and fear of separation that define DPD. |
| 16 – 30 | Mild — Some Dependent Traits | Some dependent traits present. This may reflect a supportive, relationship-oriented style rather than a disorder. Worth reflecting on whether it limits you. |
| 31 – 45 | Moderate — Significant Dependent Traits | A notable pattern of dependency and difficulty functioning independently. If it’s affecting your life, a professional conversation may help. |
| 46 – 60 | High — Strong Dependent Indicators | Strong alignment with dependent traits across multiple criteria. A professional evaluation can clarify what’s happening and open the door to effective support. |
What Causes Dependent Personality Disorder?
The causes of DPD aren’t fully established, and notably there are no genetic studies specific to DPD and its pathophysiology is unknown (StatPearls). Current understanding points to an interaction of factors. Early experiences are prominent in most accounts: overprotective or authoritarian parenting that discourages autonomy, chronic childhood illness that reinforced dependence, and early experiences that undermined the developing sense of self-efficacy. When a child is consistently taught — directly or indirectly — that they can’t manage on their own, or that independence is dangerous or disloyal, a dependent adaptation can take hold.
Temperament and biology contribute as well. Biologic vulnerabilities associated with anxiety appear relevant, and heritability studies of avoidant and dependent PD together suggest a shared genetic contribution to the anxious, submissive, insecure traits underlying both (Gjerde et al., 2012). Familial traits such as submissiveness and self-effacing behavior may be transmitted through both genes and modeling.
Cultural factors shape how dependency is expressed and judged. Some cultures and family systems reinforce deference, interdependence, and self-subordination — particularly for women — which affects both who develops the pattern and who gets diagnosed with it. This is part of why the gender difference in DPD diagnosis is genuinely contested rather than clearly a difference in true prevalence.
Treatment for Dependent Personality Disorder
DPD is treatable, and the prognosis with treatment is generally more favorable than for several other personality disorders — in part because people with DPD are usually motivated to engage and to please the therapist (which, handled well, supports the therapeutic alliance; handled poorly, can recreate the dependency within therapy itself).
Psychotherapy is the first-line treatment. Cognitive Behavioral Therapy targets the core beliefs about being helpless and ineffectual, and builds concrete skills for independent decision-making, assertiveness, and problem-solving. Psychodynamic approaches explore the developmental roots of the dependency and the relational patterns that maintain it. A central, delicate goal across approaches is fostering autonomy without triggering the person’s fear of abandonment — the therapist has to help the person stand on their own without feeling that support is being withdrawn as punishment.
Medication does not treat DPD itself, but antidepressants or anti-anxiety medication may be used for co-occurring depression or anxiety, which are common. Because DPD frequently coexists with depression, anxiety disorders, and other conditions, treating those comorbidities is often an important part of the overall picture.
A specific caution: because people with DPD can become dependent on the therapist, good treatment deliberately builds toward independence and self-efficacy rather than fostering ongoing reliance. The aim is not to strip away the person’s relationships or their capacity for healthy connection, but to expand their ability to function, decide, and cope on their own — so that connection becomes a choice rather than a perceived necessity for survival.
Frequently Asked Questions
What is dependent personality disorder?
Dependent Personality Disorder (DPD; DSM-5-TR 301.6 / F60.7) is a Cluster C personality disorder characterized by a pervasive, excessive need to be taken care of, leading to submissive and clinging behavior and intense fears of separation. People with DPD struggle to make everyday decisions without reassurance, rely on others to take responsibility for major life areas, avoid disagreement for fear of losing support, and feel helpless when alone. Diagnosis requires at least five of eight DSM-5-TR criteria, a pattern beginning by early adulthood and present across contexts. It affects roughly 0.5–0.6% of the population and is one of the less common personality disorders.
What is the difference between dependent personality disorder and codependency?
They’re often confused, but they point in opposite directions. Dependent Personality Disorder centers on the need to be taken care of — relying on others for decisions, direction, reassurance, and a sense of security. Codependency (which is not a formal DSM diagnosis but a widely used clinical and self-help concept) typically centers on compulsive caretaking of others — building identity and self-worth around being needed, often in a relationship with someone who is addicted, ill, or impaired. DPD is about receiving care; codependency is about giving it to the point of self-neglect. A person can have features of both, but they are distinct patterns. The Codependency Test covers the caretaking pattern specifically.
Is it normal to depend on other people?
Yes, completely. Healthy interdependence — relying on partners, friends, and family for support, comfort, advice, and shared decision-making — is a normal and healthy part of human life. Dependent Personality Disorder is not “needing people”; it’s a pervasive, excessive dependency that impairs functioning: difficulty making ordinary decisions alone, inability to disagree for fear of losing support, feeling helpless when alone, and organizing life around maintaining care from others at the cost of one’s own autonomy. The line is drawn by degree, pervasiveness, and impairment — and by whether the dependence is realistic for the person’s actual circumstances. Depending on people is healthy; being unable to function without them is the disorder.
What is the difference between dependent and avoidant personality disorder?
Both are Cluster C disorders rooted in anxiety and low self-confidence, but they respond in opposite ways. A person with avoidant personality disorder wants closeness but avoids relationships out of fear of rejection and criticism — they withdraw until they’re certain of uncritical acceptance. A person with dependent personality disorder actively seeks out and clings to relationships, because their fear is of being left to cope alone. One avoids connection to prevent rejection; the other attaches urgently to prevent abandonment. They share an anxious, self-doubting core (and some research suggests shared heritability), which is why they can look similar and sometimes co-occur, but the behavioral direction is reversed.
How common is dependent personality disorder?
DPD is one of the less common personality disorders, with prevalence estimates around 0.5–0.6% of the population (the National Comorbidity Survey Replication found 0.6%; NESARC data using DSM-IV criteria found 0.5%). It’s diagnosed more often in women (around 0.6%) than men (around 0.4%), though whether this reflects true prevalence or diagnostic and cultural bias is debated. DPD is more common in younger adults (about 0.9% among ages 18–29) than older adults (about 0.3% over 65), and shows little difference across racial or ethnic groups.
Can dependent personality disorder be treated?
Yes, and the outlook with treatment is relatively favorable compared to some other personality disorders, partly because people with DPD tend to be motivated and engaged in treatment. Psychotherapy is first-line: Cognitive Behavioral Therapy targets the underlying beliefs about being helpless and builds skills for independent decision-making and assertiveness, while psychodynamic therapy explores the developmental roots. Medication doesn’t treat DPD itself but may help co-occurring depression or anxiety. A key goal of good treatment is fostering autonomy and self-efficacy without triggering the person’s fear of abandonment — and deliberately avoiding recreating the dependency within the therapy relationship itself.
What causes dependent personality disorder?
The causes aren’t fully established — notably, there are no DPD-specific genetic studies and its pathophysiology is unknown. Current understanding points to an interaction of early experiences (overprotective or authoritarian parenting that discourages autonomy, chronic childhood illness, experiences that undermined self-confidence), temperamental and biologic vulnerabilities associated with anxiety, and cultural factors that reinforce deference and self-subordination. Twin research on avoidant and dependent PD together suggests a shared heritable contribution to the anxious, submissive traits underlying both. As with most personality disorders, no single cause explains it; it emerges from the interaction of temperament and developmental environment.
Related Tests
- Avoidant Personality Disorder Test — the closest Cluster C relative; both involve anxiety and low self-confidence but respond in opposite directions (avoiding vs clinging)
- Codependency Test — the caretaking counterpart often confused with DPD; centers on being needed rather than needing to be cared for
- Obsessive-Compulsive Personality Disorder Test — the third Cluster C disorder; shares the anxious/fearful core through a very different presentation
- Borderline Personality Disorder Test — BPD’s fear of abandonment overlaps with DPD’s separation fears, but through emotional instability rather than submissive dependence
- Anxiety Test — anxiety underlies DPD and commonly co-occurs; the fear of being unable to cope alone is anxiety at its core
- Clinical Depression Test — depression frequently co-occurs with DPD, especially around relationship loss and low self-efficacy
- Self-Esteem Test — low self-confidence in one’s own judgment and abilities is central to DPD; worth assessing alongside
- All Personality Disorder Tests — explore the full set of Cluster A, B, and C personality disorder screenings
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Dependent Personality Disorder 301.6 (F60.7). psychiatry.org
- Merck Manual Professional Edition. (2026). Dependent Personality Disorder (DPD). [DSM-5-TR criteria; treatment; DPD vs avoidant differential; causes] merckmanuals.com
- Ekáez, T., et al.; StatPearls. (2024). Dependent Personality Disorder. [Prevalence 0.5-0.6%; women 0.6% vs men 0.4%; age distribution; no genetic studies; unknown pathophysiology] ncbi.nlm.nih.gov
- Bornstein, R.F. (1992). The dependent personality: developmental, social, and clinical perspectives. Psychological Bulletin, 112(1), 3–23. [Cognitive-interactionist model of dependency]
- Gjerde, L.C., Czajkowski, N., Røysamb, E., et al. (2012). The heritability of avoidant and dependent personality disorder assessed by personal interview and questionnaire. Acta Psychiatrica Scandinavica, 126(6), 448–457. [Shared heritability of avoidant and dependent PD] doi.org
- Tyrer, P., Morgan, J., & Cicchetti, D. (2004). The Dependent Personality Questionnaire (DPQ): a screening instrument for dependent personality. International Journal of Social Psychiatry, 50(1), 10–17. [DPQ screening instrument]
- Wikipedia. (2026). Dependent personality disorder. [Cluster C classification; ICD-11 dimensional shift; overview] en.wikipedia.org