
There are things that happen in the mind that are genuinely difficult to name. Finding yourself somewhere without remembering how you got there. Looking back at a conversation and feeling like it happened to someone else. Being told you did or said things that have no place in your memory. Feeling like there are parts of you that operate separately from each other — with different moods, different voices, different ways of relating to the world.
These experiences are real. They are not invented, not exaggerated, not the product of too many movies about split personalities. They are recognized clinical phenomena — the core of what dissociation describes — and they exist on a spectrum from the mild and ordinary to the severe and clinically significant.
Dissociative Identity Disorder (DID) — formerly called Multiple Personality Disorder, and sometimes still referred to as split personality disorder — is the most severe form of dissociative disorder recognized in the DSM-5-TR. It is also among the most misunderstood, most stigmatized, and most frequently either dismissed or over-romanticized. This Dissociative Identity Disorder test uses the framework of the Dissociative Experiences Scale II (DES-II), the most widely validated dissociation screening instrument in clinical research, to provide a meaningful first look at your dissociation levels — not to diagnose, but to give you information worth taking seriously.
What Is Dissociative Identity Disorder?
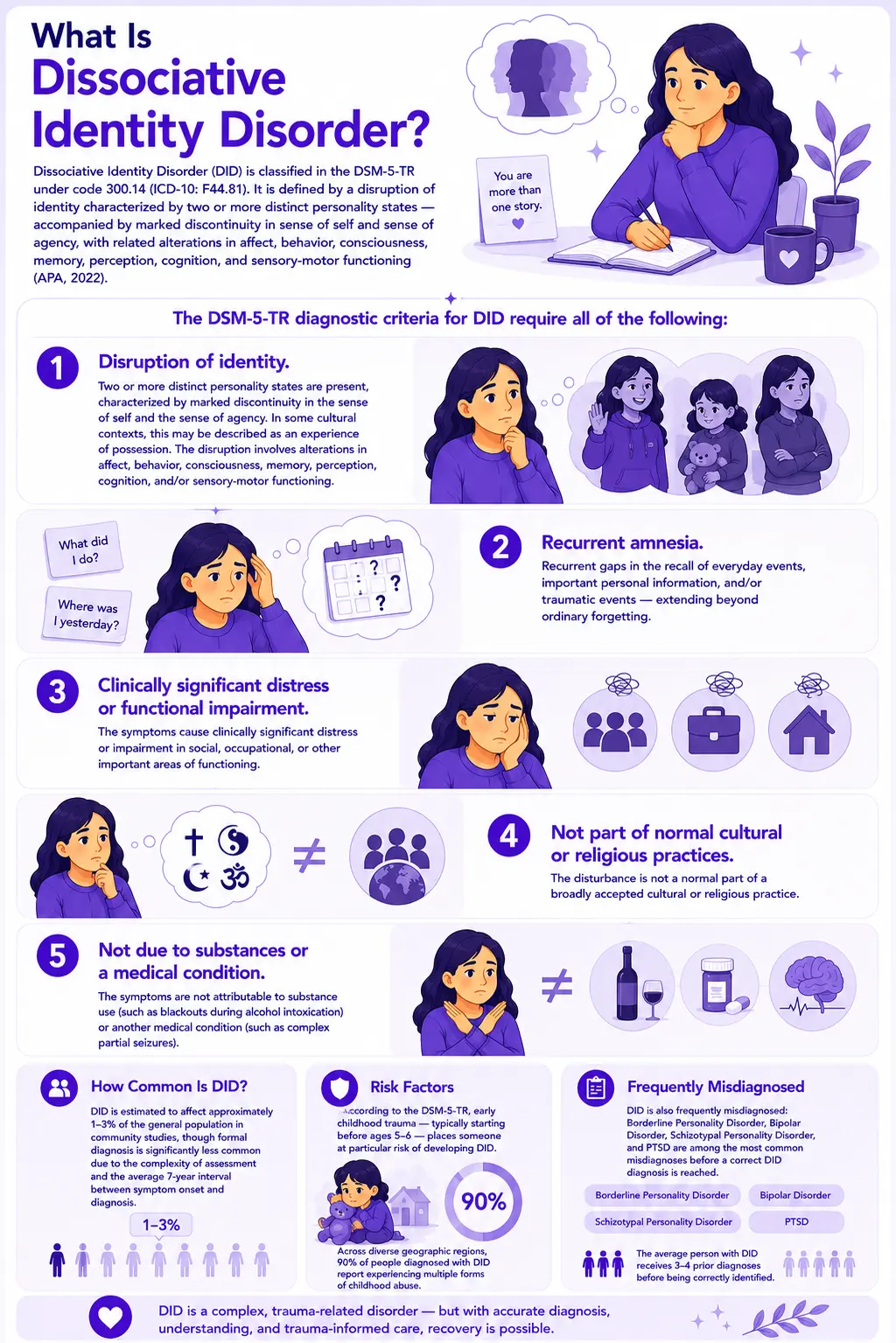
Dissociative Identity Disorder (DID) is classified in the DSM-5-TR under code 300.14 (ICD-10: F44.81). It is defined by a disruption of identity characterized by two or more distinct personality states — accompanied by marked discontinuity in sense of self and sense of agency, with related alterations in affect, behavior, consciousness, memory, perception, cognition, and sensory-motor functioning (APA, 2022).
The DSM-5-TR diagnostic criteria for DID require all of the following:
- Disruption of identity. Two or more distinct personality states are present, characterized by marked discontinuity in the sense of self and the sense of agency. In some cultural contexts, this may be described as an experience of possession. The disruption involves alterations in affect, behavior, consciousness, memory, perception, cognition, and/or sensory-motor functioning.
- Recurrent amnesia. Recurrent gaps in the recall of everyday events, important personal information, and/or traumatic events — extending beyond ordinary forgetting.
- Clinically significant distress or functional impairment. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- Not part of normal cultural or religious practices. The disturbance is not a normal part of a broadly accepted cultural or religious practice.
- Not due to substances or a medical condition. The symptoms are not attributable to substance use (such as blackouts during alcohol intoxication) or another medical condition (such as complex partial seizures).
DID is estimated to affect approximately 1–3% of the general population in community studies, though formal diagnosis is significantly less common due to the complexity of assessment and the average 7-year interval between symptom onset and diagnosis. According to the DSM-5-TR, early childhood trauma — typically starting before ages 5–6 — places someone at particular risk of developing DID. Across diverse geographic regions, 90% of people diagnosed with DID report experiencing multiple forms of childhood abuse.
DID is also frequently misdiagnosed: Borderline Personality Disorder, Bipolar Disorder, Schizotypal Personality Disorder, and PTSD are among the most common misdiagnoses before a correct DID diagnosis is reached. The average person with DID receives 3–4 prior diagnoses before being correctly identified.
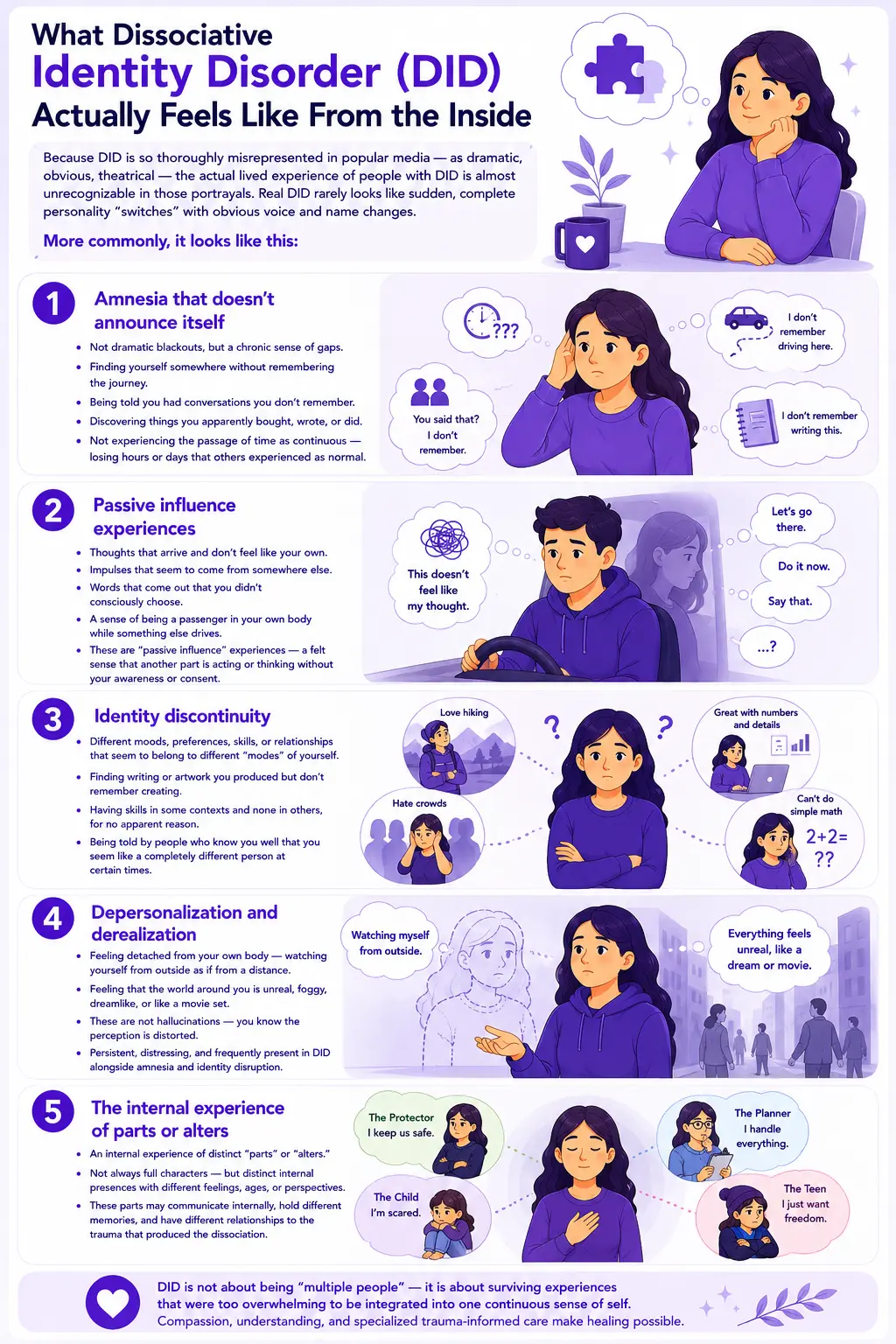
What Dissociative Identity Disorder (DID) Actually Feels Like From the Inside
Because DID is so thoroughly misrepresented in popular media — as dramatic, obvious, theatrical — the actual lived experience of people with DID is almost unrecognizable in those portrayals. Real DID rarely looks like sudden, complete personality “switches” with obvious voice and name changes. More commonly, it looks like this:
Amnesia that doesn’t announce itself. The most characteristic experience is not dramatic blackouts — it is a chronic, pervasive sense of gaps. Finding yourself somewhere without remembering the journey. Being told you had conversations you don’t remember. Discovering things you apparently bought, wrote, or did. Not experiencing the passage of time as continuous — losing hours or days that other people experienced as normal.
Passive influence experiences. Thoughts that arrive and don’t feel like your own. Impulses that seem to come from somewhere else. Words that come out of your mouth that you didn’t consciously choose. A sense of being a passenger in your own body while something else drives. These are called “passive influence” experiences — a felt sense that another part of you is acting or thinking without your awareness or consent.
Identity discontinuity. Different moods, preferences, skills, or relationships that seem to belong to different “modes” of yourself — modes that don’t always remember what the others do. Finding writing or artwork you produced but don’t remember creating. Having skills in some contexts and none in others, for no apparent reason. Being told by people who know you well that you seem like a completely different person at certain times.
Depersonalization and derealization. Feeling detached from your own body — watching yourself from outside as if from a distance, or from the ceiling. Feeling that the world around you is unreal, foggy, dreamlike, or like a movie set. These are not hallucinations — the person knows the perception is distorted — but they are persistent, distressing, and frequently present in DID alongside the amnesia and identity disruption.
The internal experience of parts or alters. Many people with DID describe an internal experience of distinct “parts” or “alters” — not always fully formed characters with different names, but distinct internal presences with different emotional tones, perspectives, ages, or ways of relating to the world. These parts may communicate internally, may hold different memories, and may have different relationships to the trauma that produced the dissociation.
About This Test — The DES-II Framework
This Dissociative Identity Disorder Test is modeled on the Dissociative Experiences Scale II (DES-II), developed by Dr. Eve Bernstein Carlson and Dr. Frank W. Putnam (1993), the most widely used and validated dissociation screening instrument in clinical and research contexts. The DES-II measures dissociative experiences across three empirically validated subscales:
- Amnestic Dissociation. Questions covering memory gaps, blackouts, and finding evidence of actions or conversations you have no recall of — the amnesia component that is central to DID diagnosis.
- Depersonalization/Derealization. Questions covering felt detachment from your own body, observing yourself from outside, and experiences of the external world as unreal or dreamlike.
- Absorption and Imaginative Involvement. Questions covering experiences of being so absorbed in internal experiences that you lose track of external reality — becoming completely lost in memories, daydreams, or internal states in ways that feel involuntary rather than chosen.
Answer each question based on how often these experiences occur for you in general — not during a specific period, but as a reflection of your overall experience pattern. The scale runs from Never to Very Often.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Very Often = 4
Total range: 0–112. This is a screening tool — it cannot diagnose DID. Only a qualified mental health professional, using a structured clinical interview and comprehensive history, can diagnose DID. A high score on this test is clinically meaningful and worth taking to a professional evaluation — specifically, a trauma-informed clinician or psychiatrist familiar with dissociative disorders.
Understanding Your DID Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 28 | Low Dissociation | Normal variation in attention and memory. Non-clinical. These experiences are within the range that most people report and are not consistent with pathological dissociation. |
| 29 – 56 | Moderate Dissociation | Elevated dissociation that may be trauma-linked. Warrants monitoring and professional discussion, particularly if there is a trauma history. |
| 57 – 112 | High Dissociation | Clinically significant dissociation. Consistent with the range where DID and other dissociative disorders are commonly found. Professional evaluation is strongly recommended. |
Am I Faking DID? Understanding Doubt and Skepticism
This question deserves its own section — because it is one of the most common and most painful questions asked by people who are genuinely experiencing dissociative symptoms. “Am I making this up?” “Is this real?” “What if I’m faking?”
The fact that you are asking whether you are faking is itself a significant piece of clinical information. People who fabricate symptoms for attention or secondary gain do not typically spend significant time in distress wondering whether their experiences are real. The relentless self-doubt, the questioning of your own reality, the sense that your experiences can’t possibly be legitimate — these are features of DID, not evidence against it. Dissociation itself disrupts the sense of continuous, trustworthy selfhood that would allow you to feel certain about your own experience.
Several factors contribute to this self-doubt:
Media misrepresentation. Popular depictions of DID as dramatic, theatrical, and obviously visible have created an impossible standard. Real DID is subtle, confusing, and frequently invisible to others. When your experience doesn’t match the movie version, it’s natural to question whether it’s real — but the movie version is not accurate.
Dissociation disrupts memory of dissociation. One of the defining features of dissociation is that it impairs your ability to remember and integrate your own experiences. This means you may genuinely not remember the episodes that your dissociation produces — and that absence of memory can make the experiences feel invented or exaggerated when you try to account for them later.
Stigma and invalidation. DID is among the most stigmatized mental health conditions. Many people with DID report years of being told their experiences are fabricated, attention-seeking, or the product of watching too much media coverage of the condition. Internalized stigma — believing the dismissals you’ve received — produces the “am I faking” question from the inside.
The influence of social media. There is genuine concern in the clinical community about DID being misrepresented and over-identified on social media platforms. This does not mean that DID is rare or that people who identify with it are fabricating symptoms. It means that self-diagnosis based on social media content is not reliable in either direction. The correct response to uncertainty is clinical evaluation, not self-dismissal.
If you are asking, “am I faking DID?” — the most honest and clinically appropriate answer is: a qualified professional can help you find out. The Structured Clinical Interview for Dissociative Disorders (SCID-D) is specifically designed to distinguish genuine dissociative experiences from other presentations and is the appropriate tool for answering this question.
DID vs. OSDD vs. Dissociation — What’s the Difference?
Not everyone who experiences significant dissociation has DID. The dissociative disorder spectrum includes several distinct conditions, and understanding where experiences fit clinically requires professional assessment.
| Feature | Normal Dissociation | PTSD with Dissociation | OSDD (Other Specific Dissociative Disorder) | DID |
|---|---|---|---|---|
| Identity disruption | None | Possible — trauma-linked derealization/depersonalization | Present but partial — parts may not fully take control | Full — two or more distinct identity states that take executive control |
| Amnesia | Absent or minimal | Trauma-specific amnesia possible | Partial — may not meet full DID amnesia criteria | Recurrent, significant — including for everyday events |
| Trauma history | Not required | Required by definition | Usually present, particularly early childhood trauma | Present in >90% of cases; typically severe, early, repeated |
| DSM-5-TR code | — | PTSD with dissociative subtype | 300.15 (F44.89) | 300.14 (F44.81) |
| Treatment approach | No treatment needed | Trauma-focused therapy (EMDR, CPT, PE) | Phase-based trauma therapy is similar to the DID approach | Phase-based therapy per ISSTD guidelines; long-term |
| PsyMed screening | No screening needed | PTSD Test | This test (DES-II based) | This test (DES-II based) |
The distinction between OSDD and DID is clinically important: OSDD — formerly called DDNOS (Dissociative Disorder Not Otherwise Specified) — involves dissociative identity disruption that is significant but does not fully meet DID criteria, typically because the identity states don’t take full executive control or because amnesia is less complete. The ICD-11 introduced the category “partial DID” to capture this presentation specifically. Both conditions respond to similar treatment approaches, and the clinical priority is identifying and treating dissociation and trauma regardless of which specific label applies.
What Causes Dissociative Identity Disorder?
The theoretical model with the strongest empirical support for DID is the trauma model, specifically the structural dissociation of personality theory developed by Van der Hart, Nijenhuis, and Steele. The core hypothesis, proposed by Putnam and colleagues, is that alternate identities result from the inability of traumatized children to develop a unified sense of self across various behavioral states — particularly when traumatic exposure begins before age 5 (StatPearls, 2023).
Severe, early, repeated childhood trauma. The foundational cause of DID in the vast majority of cases is severe, repeated trauma in early childhood — before the developing sense of self has consolidated sufficiently to integrate overwhelming experiences. Chronic physical, sexual, or emotional abuse; severe neglect; medical trauma; war exposure; cult abuse; attachment disruption; and dysfunctional family systems are all documented causes. The dissociation represents the child’s mind partitioning overwhelming experience into separate compartments — separate identity states — as a survival mechanism.
Developmental timing. The age at which trauma begins matters significantly. Children below age 5–6 are in a developmental period where the sense of a unified self is still forming. Severe trauma during this period disrupts that integration process, producing the structural dissociation that develops over time into distinct identity states. Trauma beginning in adolescence or adulthood is much less likely to produce DID — it may produce PTSD, but not typically the identity fragmentation characteristic of DID.
Absence of protective factors. DID is more likely to develop when trauma occurs in the context of an attachment relationship (perpetrated by caregivers), when there is no safe adult to turn to, and when the child has no opportunity to process or make sense of the traumatic experience. The isolation and secrecy that frequently accompany childhood abuse create conditions where dissociation becomes the primary (and only) survival strategy.
Comorbidities. DID rarely presents alone. The most common comorbidities are PTSD, major depressive disorder, anxiety disorders, Borderline Personality Disorder, somatic symptom disorders, and eating disorders. Substance use disorders frequently develop as self-medication for dissociative and trauma symptoms. Depersonalization/Derealization Disorder symptoms are frequently present and may represent a separate diagnosis or a feature of the DID presentation.
Treatment for Dissociative Identity Disorder
DID is a treatable condition. Meaningful functional improvement is achievable, and complete or substantial integration is possible for many people who receive appropriate, sustained treatment. The International Society for the Study of Trauma and Dissociation (ISSTD) published treatment guidelines (most recently updated in 2011, with ongoing revisions) that represent the clinical standard of care.
Phase 1: Safety, stabilization, and symptom reduction. The first and often longest phase of treatment focuses not on trauma processing but on building safety and stability. This includes developing internal communication between identity states, reducing self-destructive behaviors, building coping and affect regulation skills, and establishing a stable, trusting therapeutic relationship. Phase 1 can take months to years and is often where the majority of clinical work occurs. Rushing to trauma processing before stabilization is well-established is known to destabilize treatment.
Phase 2: Working through traumatic memories. Once sufficient stabilization is established, trauma-focused work begins — processing the memories and experiences that produced the dissociation. This is done carefully and collaboratively with all parts of the system. Approaches adapted for DID include EMDR modified for dissociative presentations, parts-based approaches (Internal Family Systems, ego state therapy), and phase-oriented trauma therapy.
Phase 3: Integration and rehabilitation. The final phase involves integrating what has been processed into a more cohesive sense of self and identity, and building toward the functional life the person wants. For some people, this involves the fusion of identity states into a unified sense of self; for others, it involves a cooperative, functional relationship between parts without full fusion. Both are valid treatment outcomes.
Medication. No medications are specifically approved for DID. Pharmacotherapy is used adjunctively to address comorbid conditions — antidepressants for depression, anxiolytics for anxiety, prazosin for PTSD nightmares — but does not directly address the dissociation or identity fragmentation. Low-dose antipsychotics are sometimes used for perceptual disturbances. Medication decisions should be made by a psychiatrist familiar with dissociative disorders.
Finding appropriate treatment. Not all therapists are trained in dissociative disorders. The ISSTD (isstd.org) maintains a clinician finder for trauma and dissociation specialists. When seeking treatment, explicitly ask whether the clinician has training and experience with DID and complex trauma — and whether they are familiar with the ISSTD treatment guidelines.
Frequently Asked Questions
What is Dissociative Identity Disorder (DID)?
Dissociative Identity Disorder (DID) — formerly called Multiple Personality Disorder and sometimes referred to as split personality disorder — is a DSM-5-TR recognized condition (300.14 / F44.81) characterized by the presence of two or more distinct identity states, recurrent amnesia for everyday events and personal information, and significant distress or functional impairment. It develops primarily as a response to severe, repeated childhood trauma before approximately age 5–6, when the developing sense of self is unable to integrate overwhelming experience into a unified identity. DID affects an estimated 1–3% of the general population and has an average of 7 years between symptom onset and correct diagnosis.
What is the difference between DID and Multiple Personality Disorder?
They are the same condition under different names. “Multiple Personality Disorder” was the name used in DSM-III (1980–1994). The DSM-IV (1994) renamed it to Dissociative Identity Disorder to better reflect the clinical understanding of the condition — that it involves disruption of identity and dissociation rather than literally separate “personalities.” The informal term “split personality disorder” is also sometimes used, but is not a clinical term. All three refer to the same condition as currently defined in DSM-5-TR.
Is DID real? Isn’t it controversial?
DID is a real, DSM-5-TR recognized condition with decades of clinical and research documentation. It is also genuinely controversial in some academic and clinical communities — the debate centers not on whether dissociation and trauma produce identity disruption (which is well-established) but on questions of cultural influence, iatrogenic factors in some historical presentations, and diagnostic reliability. A 2024 review in Progress in Neurology and Psychiatry notes that DID remains an area of clinical debate while affirming its recognition in both DSM-5 and ICD-11. The controversy does not negate the reality of the experiences of people with DID — it reflects ongoing academic discussion about classification and diagnosis, not a dismissal of dissociative phenomena.
Can I develop DID from watching social media about DID?
This is a genuine clinical concern. There is evidence that social media exposure to DID content can influence how people describe and present dissociative symptoms, and clinical organizations have raised concerns about over-identification with DID labels based on social media content rather than clinical assessment. This does not mean that everyone who identifies with DID after seeing social media content is fabricating symptoms — many people first recognize their real experiences through online communities. It means that social media is not a reliable diagnostic tool, and that clinical evaluation by a trained professional is the appropriate path to understanding whether and what dissociative disorder is present.
How is DID diagnosed?
DID is diagnosed through a comprehensive clinical assessment — not through questionnaires or online tests. The gold standard diagnostic instrument is the Structured Clinical Interview for Dissociative Disorders (SCID-D), which provides a structured evaluation of all five core dissociative symptoms: amnesia, depersonalization, derealization, identity confusion, and identity alteration. Diagnosis requires a trained mental health professional — ideally a psychiatrist or psychologist familiar with trauma and dissociative disorders — who takes a comprehensive history and rules out other conditions. The average person with DID receives 3–4 prior diagnoses (most commonly BPD, bipolar disorder, or schizophrenia) before being correctly identified.
What is the difference between DID and BPD?
This is one of the most clinically important distinctions, as the two conditions share several surface features and frequently co-occur. Borderline Personality Disorder (BPD) involves emotional dysregulation, identity disturbance, fear of abandonment, and unstable relationships — but the identity disturbance in BPD is characterized by a diffuse, shifting sense of self, not by distinct identity states with separate memory systems. DID involves structured dissociation between discrete identity states with amnesia across states. Both conditions frequently have a trauma history, and they can co-occur — making clinical differentiation important and sometimes complex. The BPD Test is worth completing if BPD features are prominent alongside dissociative symptoms.
What does the DES-II measure?
The Dissociative Experiences Scale II (DES-II), developed by Dr. Eve Bernstein Carlson and Dr. Frank W. Putnam (1993), is the most widely used dissociation screening instrument in clinical research. It measures three domains of dissociative experience: amnestic dissociation (memory gaps and blackouts), depersonalization/derealization (detachment from self or reality), and absorption/imaginative involvement (involuntary absorption in internal experiences). Research using the DES-II has established that people with DID typically score above 60–70 on the full scale. The DES-II is a screening tool — high scores indicate that further clinical assessment is warranted, not that DID is present.
Related Tests
DID and dissociative disorders rarely present in isolation. These are the most clinically relevant companion assessments:
- PTSD Test — PTSD and DID share trauma origins and frequently co-occur; PTSD with dissociative subtype is an important related presentation
- Depersonalization/Derealization Disorder Test — depersonalization and derealization are core DID features but also exist as standalone conditions; important to assess separately
- Borderline Personality Disorder Test — one of the most common DID misdiagnoses; both involve identity disturbance, both frequently have trauma histories, and both require different treatment approaches
- Clinical Depression Test — major depressive disorder is the most common DID comorbidity; frequently part of the presenting picture
- Anxiety Test — anxiety disorders are common DID comorbidities; often part of the trauma-based symptom complex
- Schizotypal Personality Disorder Test — DID is sometimes misdiagnosed as schizophrenia or schizotypal PD due to overlapping perceptual experiences; an important diagnostic distinction
- Bipolar Test — bipolar disorder is a common DID misdiagnosis; mood variability in DID may appear similar to bipolar cycling
- ADHD Test — ADHD and dissociation share attention and concentration difficulties; DID is sometimes misdiagnosed as ADHD in children
For more dissociation and psychosis screenings, visit our Dissociation and Psychosis collection.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Dissociative Identity Disorder 300.14 (F44.81). psychiatry.org
- Carlson, E.B. & Putnam, F.W. (1993). An update on the Dissociative Experiences Scale. Dissociation, 6(1), 16–27. [Foundational DES-II validation paper]
- Brand, B.L., Schielke, H.J., Putnam, K., et al. (2025). A randomized controlled trial assists individuals with complex trauma and dissociation in Finding Solid Ground. Psychological Trauma. doi:10.1037/tra0001871. msdmanuals.com
- StatPearls. (2023). Dissociative Identity Disorder. NBK568768. ncbi.nlm.nih.gov
- Young, et al. (2024). Dissociative identity disorder: a review of the diagnosis that divides. Progress in Neurology and Psychiatry. onlinelibrary.wiley.com
- Wikipedia. (2025). Dissociative identity disorder. en.wikipedia.org
- MSD Manual Professional Edition. (2025). Dissociative Identity Disorder. msdmanuals.com
- HealthyPlace. (2022). Dissociative Identity Disorder (DID) DSM-5 Criteria. healthyplace.com
- International Society for the Study of Trauma and Dissociation. (2011). Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision. isstd.org
- Trauma and Dissociation. (2015). Dissociative Identity Disorder Signs, Symptoms and DSM-5 Criteria. traumadissociation.com