
If you’re struggling with an eating disorder, support is available.
📞 National Alliance for Eating Disorders Helpline — 1-866-662-1235 (daytime hours, staffed by licensed therapists)
💬 Crisis Text Line — Text “NEDA” to 741741 for 24/7 crisis support
If you’re in immediate danger or crisis, call or text 988 (Suicide & Crisis Lifeline). Eating disorders are serious and treatable — reaching out early makes a real difference.
Our relationship with food is complicated, and worrying about it doesn’t automatically mean you have an eating disorder. But eating disorders are also more common — and more varied — than many people realize, and they don’t always look the way we expect. They aren’t a choice, a phase, or a matter of willpower; they’re serious mental health conditions that can affect anyone, of any age, gender, body size, or background. And they are treatable, especially when caught early.
This free, confidential eating disorder test screens for patterns of disordered eating and attitudes toward food and body image that are associated with the main types of eating disorders. It won’t diagnose you — only a qualified professional can do that — but it can help you understand whether what you’re experiencing is worth taking seriously and bringing to someone who can help. 15 questions, private results.
What Is an Eating Disorder?
Eating disorders are serious mental health conditions, recognized in the DSM-5-TR, that involve persistent disturbances in eating behaviors along with distressing thoughts and emotions about food, eating, weight, or body shape. They exist on a spectrum of severity, and they can have serious effects on physical health, emotional wellbeing, and daily functioning. Crucially, they are not fundamentally about food — food and eating become the arena for deeper struggles involving control, coping, self-worth, emotion, and distress.
A vital point that the stereotypes get wrong: eating disorders affect people of every gender, age, body size, race, and background. Someone does not have to look a particular way to have one — many people with serious eating disorders are not visibly underweight, and the assumption that they must be causes countless cases to be missed. If your relationship with food and your body is causing you distress or taking up an outsized place in your life, that matters regardless of how you look.
Eating disorders are common and serious. They affect tens of millions of people, and anorexia nervosa carries the highest mortality rate of any psychiatric disorder — which is part of why early recognition matters so much. The encouraging counterpart to that sobering fact is that eating disorders are treatable, and recovery is genuinely possible, particularly when help comes early.
The Main Types of Eating Disorders
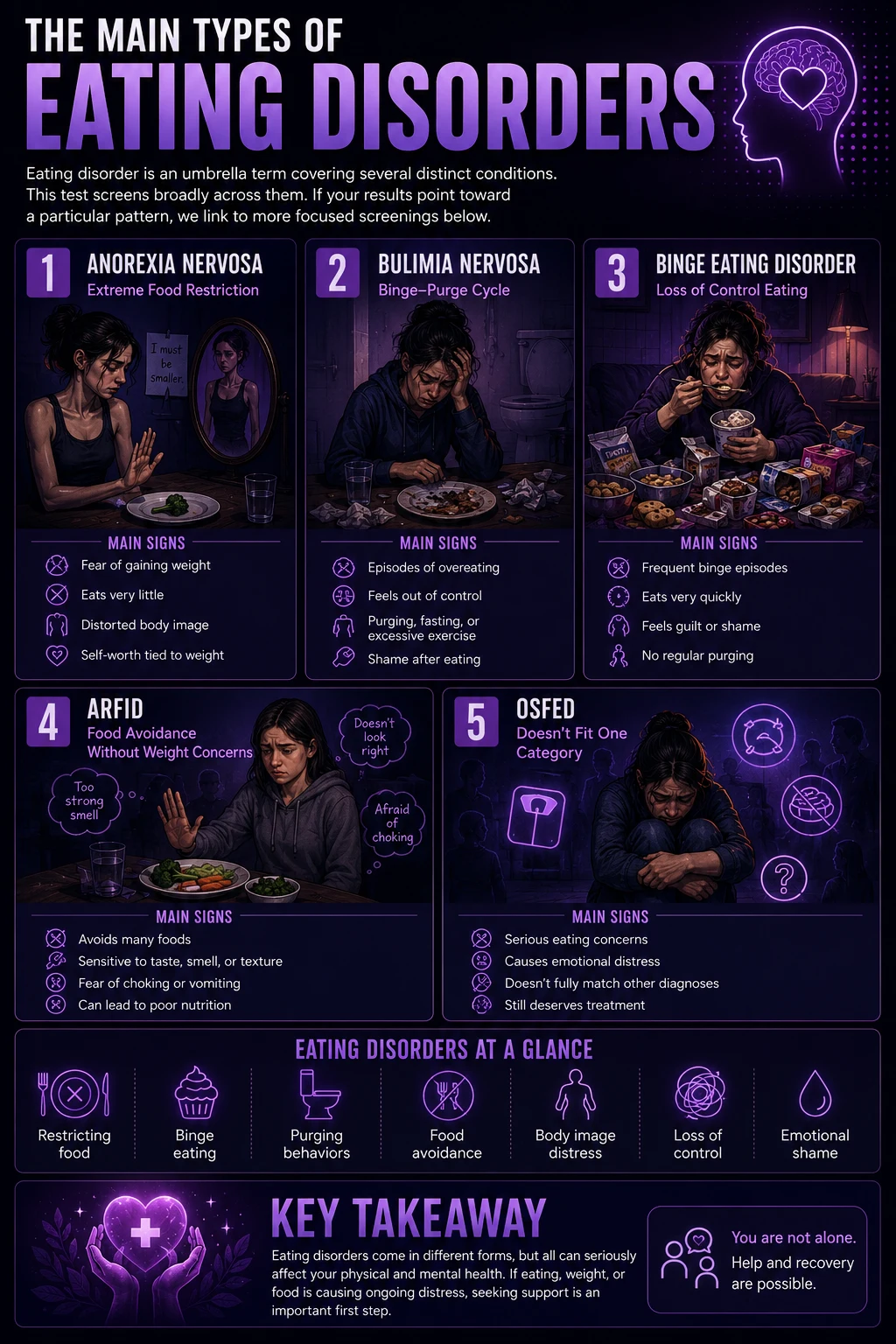
“Eating disorder” is an umbrella term covering several distinct conditions. This test screens broadly across them; if your results point toward a particular pattern, we link to more focused screenings below.
Anorexia nervosa involves restriction of food intake, an intense fear of weight gain, and a disturbance in how one experiences their body — often alongside a self-worth that has become heavily tied to body shape. It can occur across body sizes (in “atypical anorexia,” all features are present without the person being underweight). Our Anorexia Test specifically screens for this.
Bulimia nervosa involves cycles of binge eating followed by compensatory behaviors intended to counteract the eating (such as purging, fasting, or driven exercise), together with self-worth heavily influenced by body shape and weight. The cycle is typically accompanied by a sense of loss of control and significant shame.
Binge eating disorder (BED) — the most common eating disorder — involves recurrent episodes of eating large amounts with a sense of loss of control, distress, and shame, but without the regular compensatory behaviors seen in bulimia. Our Binge Eating Disorder Test screens for this specifically.
ARFID (Avoidant/Restrictive Food Intake Disorder) involves avoiding or restricting food, but — unlike anorexia — not driven by concerns about weight or body shape. Instead, it’s driven by a lack of interest in eating, sensory sensitivity to how food looks, tastes, or smells, or fear of an aversive consequence like choking. It can cause serious nutritional and functional problems.
OSFED (Other Specified Feeding or Eating Disorder) is a real and serious category for presentations that cause significant distress and impairment but don’t fit neatly into the above — which is very common. Not fitting a stereotype does not mean a problem isn’t serious or doesn’t deserve help.
Signs You Might Have an Eating Disorder
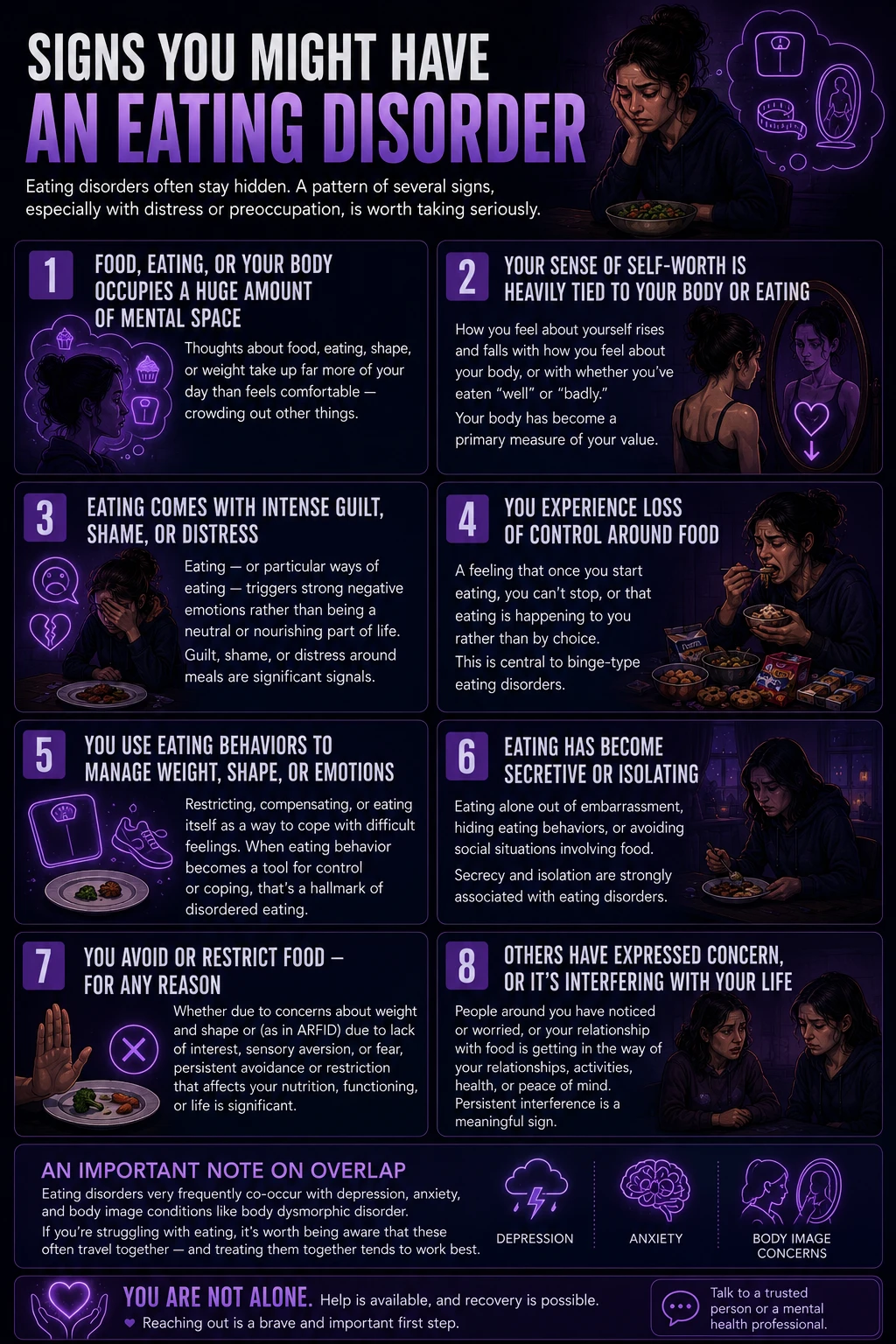
Eating disorders often stay hidden — from others, and sometimes from ourselves — behind rationalizations, secrecy, and shame. These are the signs most consistently associated with disordered eating across the different types. Because eating disorders vary so much, not every sign applies to every person; a pattern of several, especially with distress or preoccupation, is what’s worth taking seriously.
Food, eating, or your body occupies a huge amount of mental space. Thoughts about food, eating, shape, or weight take up far more of your day than they used to or than feels comfortable — crowding out other things and following you into moments that have nothing to do with eating. This preoccupation is one of the most common threads across eating disorders.
Your sense of self-worth is heavily tied to your body or eating. How you feel about yourself as a person rises and falls with how you feel about your body, or with whether you’ve eaten “well” or “badly.” Your body has become a primary measure of your value.
Eating comes with intense guilt, shame, or distress. Eating — or particular ways of eating — triggers strong negative emotions rather than being a neutral or nourishing part of life. Guilt after eating, shame about what or how much you ate, or distress around meals are significant signals.
You experience loss of control around food. A feeling that once you start eating, you can’t stop, or that eating is happening to you rather than by choice. This loss-of-control experience is central to binge-type eating disorders and is distressing in its own right.
You use eating behaviors to manage weight, shape, or emotions. Patterns aimed at controlling your body or at coping with difficult feelings — whether through restricting, through compensating for eating, or through eating itself as emotional regulation. When eating behavior becomes a tool for control or coping, that’s a hallmark of disordered eating.
Eating has become secretive or isolating. Eating alone because of embarrassment, hiding eating behaviors from others, or avoiding social situations involving food. Secrecy and isolation around eating are strongly associated with eating disorders and tend to deepen the problem.
You avoid or restrict food — for any reason. Whether driven by concerns about weight and shape or (as in ARFID) by lack of interest, sensory aversion, or fear, persistent avoidance or restriction that affects your nutrition, functioning, or life is significant.
Others have expressed concern, or the pattern is interfering with your life. People around you have noticed or worried, or your relationship with food is getting in the way of your relationships, activities, health, or peace of mind. Both external concern and functional interference are meaningful signs — especially the sense that this has become persistent rather than passing.
An important note on overlap: eating disorders very frequently co-occur with depression, anxiety, and body image conditions like body dysmorphic disorder. If you’re struggling with eating, it’s worth being aware that these often travel together — and treating them together tends to work best.
How This Test Works
This test contains 15 questions about your recent patterns, feelings, and attitudes around food, eating, and body image — drawn broadly from the features of the main eating disorders. For each, choose how often it has applied to you over the past few months: Never, Rarely, Sometimes, Often, or Always.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Your answers add up to a score from 0 to 60. This is a screening tool that looks at general patterns of disordered eating — it deliberately does not ask about or display any numbers related to weight, food amounts, or your body, because those specifics aren’t needed to recognize a problem and can be unhelpful to dwell on. Answer honestly based on your recent experience. This is not a diagnosis, and a lower score does not rule out a problem worth discussing — if you’re concerned, that concern is worth bringing to a professional regardless of your score.
Understanding Your Results
A note before your result: this screening reflects how many disordered-eating patterns you’re currently experiencing and how often. It is not a diagnosis, and eating disorders are too varied for any short quiz to capture perfectly. Please read your result as information, not a verdict — and if you’re worried, reach out regardless of where you land.
| Score Range | Level | What It Suggests |
|---|---|---|
| 0 – 15 | Few Signs | Few signs of disordered eating in your responses. If you still have specific concerns, they remain worth discussing. |
| 16 – 30 | Some Signs | Some patterns worth paying attention to. A good point to reflect and, if they’re causing distress, to talk with someone. |
| 31 – 45 | Notable Signs | A notable pattern of disordered eating. Reaching out to a professional for a proper assessment is recommended. |
| 46 – 60 | Strong Signs | A strong pattern of disordered eating. We encourage you to reach out to a professional or the Alliance helpline soon. |
What Causes Eating Disorders?
Eating disorders arise from a complex interaction of factors — there is no single cause, and importantly, they are not caused by vanity, a lack of willpower, or a person’s choice. Contributing factors include genetics and biology (eating disorders run in families and involve heritable temperamental traits and brain differences), psychological factors (perfectionism, difficulty with emotions, low self-esteem, anxiety, a need for control, and trauma), and social and cultural factors (pervasive pressures around appearance, weight stigma, and the idealization of particular body types).
Eating disorders also very commonly co-occur with other mental health conditions — particularly depression, anxiety disorders, obsessive-compulsive patterns, and trauma-related conditions. Often the eating disorder and the co-occurring condition feed each other, which is why effective treatment addresses the whole person rather than food alone. Understanding this bigger picture matters because it removes blame: an eating disorder is something a person develops through forces largely outside their control, not something they choose or could simply decide to stop.
How Eating Disorders Are Treated
Eating disorders are treatable, and a range of evidence-based approaches genuinely help. Because these conditions affect both mind and body, treatment is usually a coordinated effort. Psychological therapy is central — approaches with strong evidence include Cognitive Behavioral Therapy adapted for eating disorders (CBT-E), Family-Based Treatment (especially effective for adolescents), and other specialized modalities. Because eating disorders have real physical effects, medical monitoring and support from professionals with eating-disorder expertise are important parts of care, as is support around nutrition provided by qualified specialists within a treatment team. When co-occurring conditions like depression or anxiety are present, treating them alongside the eating disorder improves outcomes.
The single most important message is that recovery is possible. Eating disorders can feel all-consuming and permanent from the inside, but people do recover — fully — and the earlier treatment begins, the better the outcomes tend to be. Reaching out is not a sign of weakness or an overreaction; it’s the step that makes everything else possible. If you don’t know where to start, the National Alliance for Eating Disorders helpline (1-866-662-1235) is a good first call.
Frequently Asked Questions
Can this test diagnose an eating disorder?
No. This is a screening and self-reflection tool, not a diagnostic instrument. It can help you recognize whether your patterns around food, eating, and body image align with the signs of an eating disorder, and whether it’s worth seeking a professional assessment — but only a qualified healthcare professional can diagnose an eating disorder through a comprehensive evaluation. Importantly, a low score here doesn’t rule out a problem: eating disorders are varied, and if you’re concerned about your relationship with food, that concern is worth bringing to a professional regardless of what this test suggests.
Do I have to be underweight to have an eating disorder?
No — this is one of the most harmful myths about eating disorders. People of every body size can have serious eating disorders. Many people with anorexia-type restriction are not underweight (a presentation sometimes called “atypical anorexia”), and conditions like bulimia and binge eating disorder often occur in people whose bodies look unremarkable to others. Body size is not a reliable indicator of whether someone has an eating disorder or of how serious it is. If your relationship with food and your body is causing distress or dominating your life, that matters regardless of your appearance — and it deserves support.
What are the main types of eating disorders?
The main DSM-5-TR eating disorders include anorexia nervosa (restriction, fear of weight gain, body-image disturbance), bulimia nervosa (binge-and-compensate cycles with loss of control), binge eating disorder (recurrent loss-of-control eating without regular compensation — the most common), and ARFID (food avoidance or restriction driven by disinterest, sensory issues, or fear rather than body-image concerns). There’s also OSFED (Other Specified Feeding or Eating Disorder), a serious category for significant presentations that don’t fit neatly into the others. Not fitting a stereotype doesn’t make a problem less real or less deserving of help.
How common are eating disorders?
Eating disorders are common, affecting tens of millions of people. They can occur at any age and in any gender, though rates and presentations vary. They’re also frequently under-recognized and under-treated — partly because of stigma, partly because of myths (like the belief that someone must look a certain way), and partly because shame and secrecy keep many people from seeking help. This under-recognition is one reason screening tools and open conversation matter: many people who could benefit from treatment never get identified.
What is the SCOFF questionnaire?
The SCOFF is a brief, validated five-question screening tool for eating disorders, widely used by clinicians to quickly flag people who may need a fuller assessment. It has good overall accuracy (a meta-analysis of 25 studies found pooled sensitivity around 86% and specificity around 83%), and a score of two or more “yes” answers indicates a likely eating disorder warranting further evaluation. Its main limitation is that it was designed around anorexia and bulimia, so it can miss binge eating disorder, ARFID, and other presentations. This test draws on the same core concepts as the SCOFF but casts a broader net across the different types of eating disorders — though, like the SCOFF, it’s a screen, not a diagnosis.
Where can I get help for an eating disorder?
A good first step is talking with a doctor or a mental health professional, ideally one with eating-disorder expertise, who can assess what’s happening and connect you with appropriate care. In the US, the National Alliance for Eating Disorders operates a helpline — 1-866-662-1235 — staffed by licensed therapists who can help you understand your options and find treatment referrals; it’s a good place to start if you’re not sure where to turn. For crisis support, you can text “NEDA” to 741741 (Crisis Text Line) any time, or call or text 988 if you’re in crisis or having thoughts of self-harm. Reaching out early genuinely improves outcomes, and you don’t have to have everything figured out before you make that first call.
Is it possible to fully recover from an eating disorder?
Yes. Recovery is genuinely possible, and many people recover fully and go on to have a healthy, unburdened relationship with food and their bodies. Eating disorders can feel permanent and all-consuming from the inside, but they respond to treatment — especially when help begins earlier. Recovery isn’t always quick or linear, and support along the way matters, but the core message is one of real hope: an eating disorder does not have to be a life sentence, and the step that begins recovery is usually as simple, and as hard, as telling one person and asking for help.
Related Tests
- Anorexia Test — a focused screen for restriction, fear of weight gain, and body-image disturbance if your results point toward an anorexia-type pattern
- Binge Eating Disorder Test — a focused screen for recurrent loss-of-control eating without compensatory behaviors, the most common eating disorder
- Body Dysmorphic Disorder Test — for appearance-related preoccupation and distress, which frequently overlaps with eating disorders
- Clinical Depression Test — depression very commonly co-occurs with eating disorders and often needs treating alongside
- Anxiety Test — anxiety frequently accompanies and reinforces disordered eating; worth screening together
- Self-Esteem Test — self-worth tied to body and eating is central to many eating disorders; low self-esteem often travels with them
- OCD Test — obsessive-compulsive patterns overlap with the rigid, ritualized thinking that can appear in eating disorders
References
- Morgan, J.F., Reid, F., & Lacey, J.H. (1999). The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ, 319(7223), 1467–1468. [Original SCOFF development] bmj.com
- Kutz, A.M., Marsh, A.G., Gunderson, C.G., et al. (2020). Eating Disorder Screening: a Systematic Review and Meta-analysis of the SCOFF. Journal of General Internal Medicine, 35, 885–893. [Pooled sensitivity 0.86, specificity 0.83 across 25 studies] springer.com
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Feeding and Eating Disorders. psychiatry.org
- National Alliance for Eating Disorders. What Is the History and Efficacy of the SCOFF Screening Tool? [SCOFF limitations re: BED/ARFID/OSFED; helpline 1-866-662-1235] allianceforeatingdisorders.com
- Solmi, F., Hatch, S.L., Hotopf, M., et al. (2015). Validation of the SCOFF questionnaire for eating disorders in a multiethnic general population sample. International Journal of Eating Disorders, 48(3), 312–316. [Population-level performance and limitations] onlinelibrary.wiley.com