
Trauma changes the brain. For most people, the distress that follows a traumatic event gradually fades — the memories lose their raw edge, the hypervigilance quiets, the intrusions become less frequent. For others, the processing gets stuck. The memories don’t move into the past the way ordinary memories do — they stay present, visceral, and intrusive. They arrive unbidden. They disrupt sleep. They make certain places, sounds, or people feel dangerous in ways that are difficult to explain and impossible to simply dismiss.
Post-Traumatic Stress Disorder is not a sign of weakness. It is the neurobiological aftermath of an overwhelming experience — specifically, the failure of the brain’s normal memory consolidation processes to move a traumatic memory into narrative storage, instead keeping it in the sensory, arousal-linked state in which it was originally encoded. Understanding that there is a mechanism — that what you are experiencing is a known, recognized, extensively researched clinical condition — is the beginning of being able to address it.
This free PTSD Test is based on the PCL-5 (PTSD Checklist for DSM-5), the most widely used and extensively validated self-report measure of PTSD symptoms, developed by Dr. Frank Weathers and colleagues (2013) at the National Center for PTSD, U.S. Department of Veterans Affairs. 20 questions. Based on the past month. Instant, private results.
If you are currently in crisis or experiencing thoughts of self-harm, please reach out immediately. Call or text 988 (Suicide and Crisis Lifeline, United States, 24/7) or go to your nearest emergency room.
What Is PTSD?
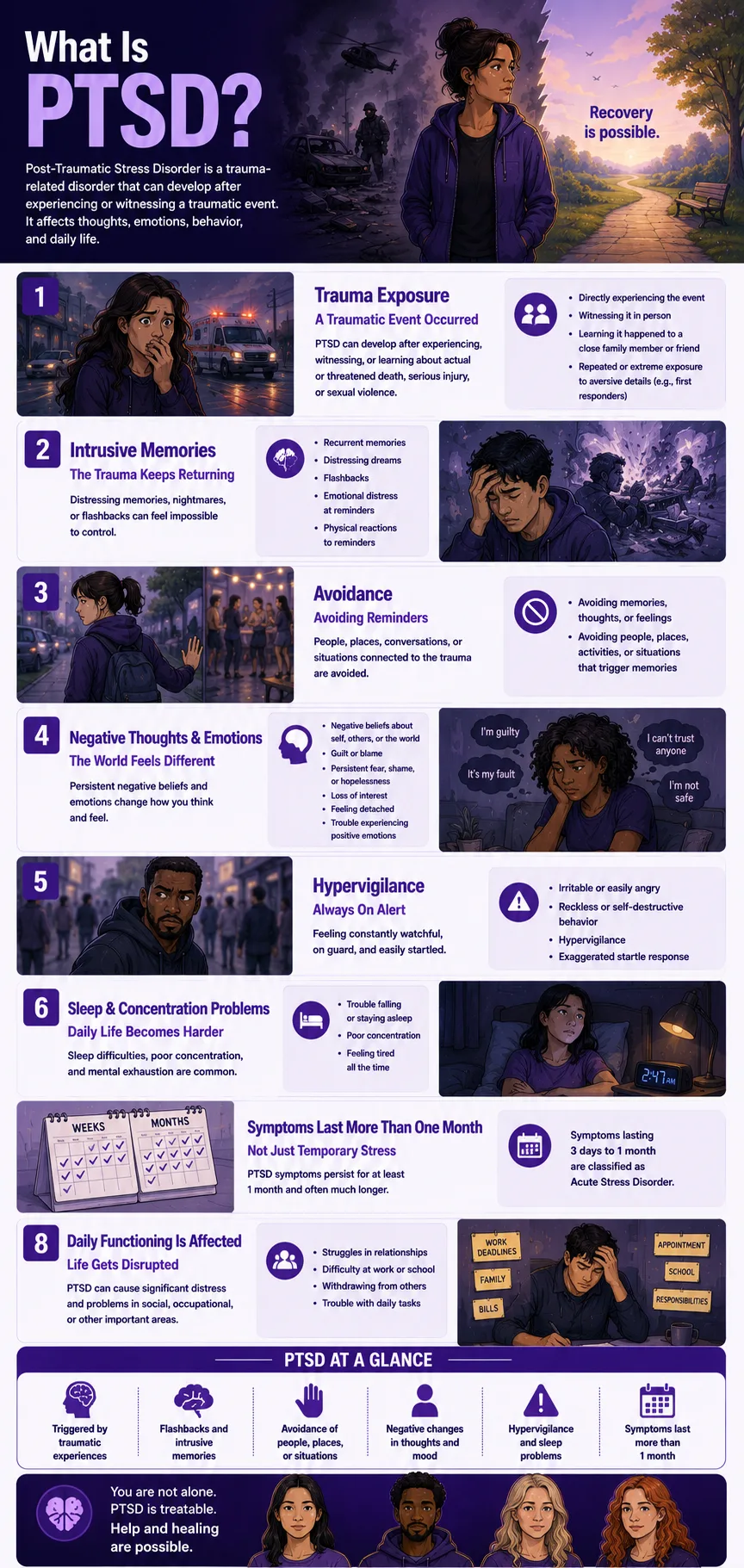
Post-Traumatic Stress Disorder (PTSD) is a Trauma- and Stressor-Related Disorder (DSM-5-TR code 309.81 / ICD-10: F43.10) that can develop after exposure to actual or threatened death, serious injury, or sexual violence. It is characterized by four symptom clusters: intrusive re-experiencing of the trauma, persistent avoidance of trauma-related stimuli, negative alterations in cognition and mood, and marked alterations in arousal and reactivity (APA, 2022).
Approximately 6% of U.S. adults will experience PTSD at some point in their lives, and around 5% — roughly 13 million Americans — are affected in any given year (National Center for PTSD, 2024). Women are twice as likely to develop PTSD as men: 8% lifetime prevalence for women versus 4% for men (National Center for PTSD, 2024). Globally, while approximately 70% of people will experience a potentially traumatic event in their lifetime, only about 5.6% go on to develop PTSD (WHO, 2024). Sexual assault carries the highest conditional risk of PTSD of any trauma type — higher than combat, accidents, or other violent trauma (WHO World Mental Health Surveys, Kessler et al., 2017).
The DSM-5-TR (APA, 2022) made no changes to the adult PTSD criteria from DSM-5 (2013). The complete DSM-5-TR diagnostic criteria for PTSD require all of the following:
Criterion A — Trauma Exposure. The person was exposed to actual or threatened death, serious injury, or sexual violence through: directly experiencing the event; witnessing it in person; learning it occurred to a close family member or friend (must have been violent or accidental); or repeated/extreme exposure to aversive details (e.g., first responders).
Criterion B — Intrusion Symptoms (≥1 required). Recurrent, involuntary, distressing memories; recurrent distressing dreams related to the trauma; dissociative reactions (flashbacks) in which the event feels like it is happening again; intense psychological distress at trauma-related cues; marked physiological reactions to trauma-related cues.
Criterion C — Avoidance (≥1 required). Persistent avoidance of distressing memories, thoughts, or feelings about the trauma; persistent avoidance of external reminders — people, places, conversations, activities, objects, or situations that trigger memories.
Criterion D — Negative Alterations in Cognition and Mood (≥2 required). Inability to remember important aspects of the trauma; persistent negative beliefs about oneself, others, or the world; persistent distorted blame of self or others; persistent negative emotional states; diminished interest in activities; feelings of detachment from others; persistent inability to experience positive emotions.
Criterion E — Alterations in Arousal and Reactivity (≥2 required). Irritable or aggressive behavior; reckless or self-destructive behavior; hypervigilance; exaggerated startle response; problems with concentration; sleep disturbance.
Criterion F — Duration: more than 1 month. (Symptoms lasting 3 days to 1 month are classified as Acute Stress Disorder.)
Criterion G — Functional Impairment. Causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Criterion H — Not attributable to substances or another condition.
Signs You Might Have PTSD
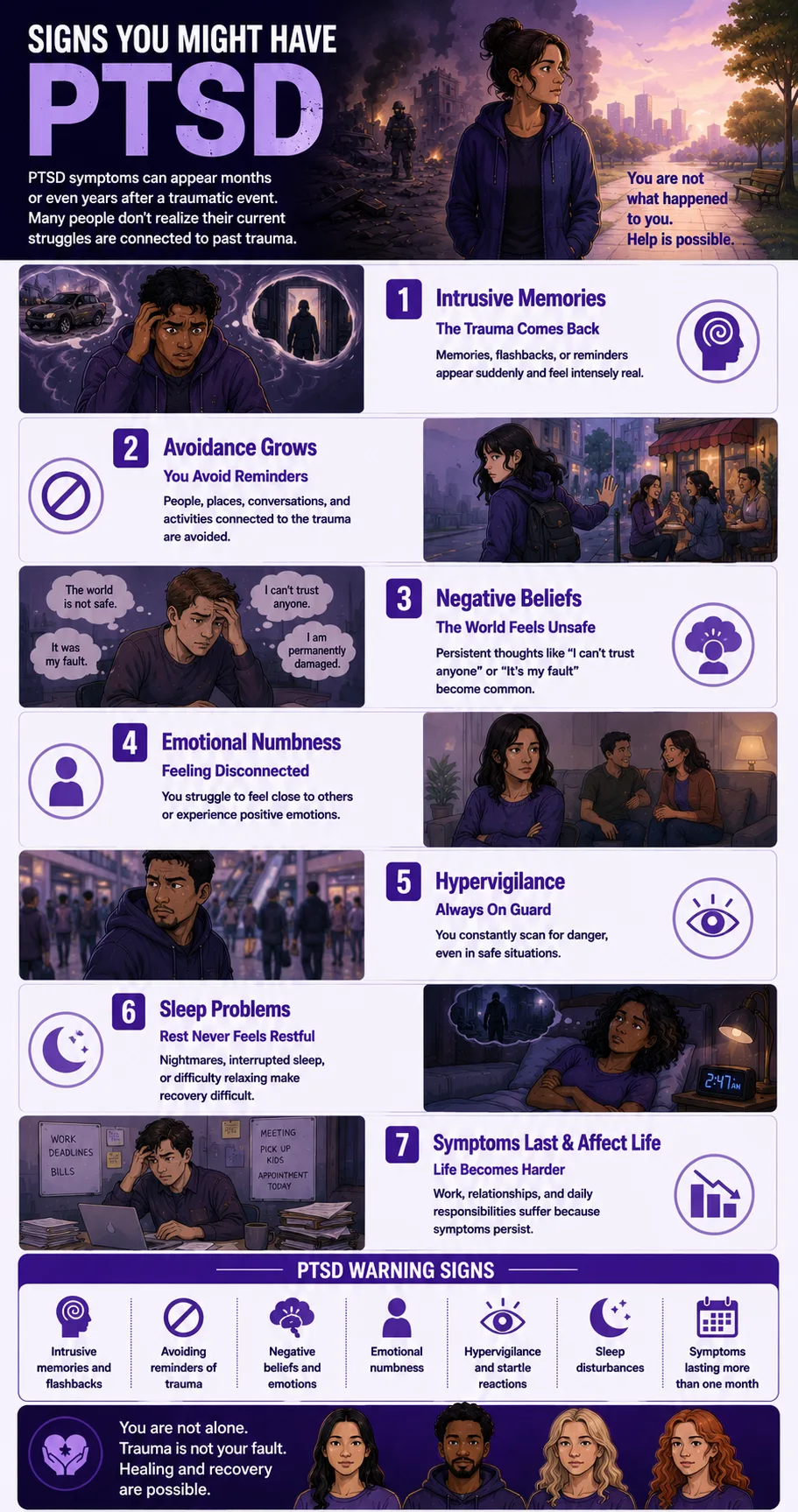
PTSD is among the most under-recognized conditions in mental health — partly because its symptoms overlap with depression and anxiety, partly because the avoidance that defines it extends to seeking help, and partly because many people don’t connect their current symptoms to a trauma that may have happened years ago. These are the patterns that most consistently indicate PTSD may be present:
Memories of the trauma arrive without your choosing them. Not when you sit down to think about what happened — but unbidden, in the middle of ordinary life. A sound, a smell, a particular quality of light, a phrase in a conversation — and suddenly you are back in it. The intrusive memories of PTSD are qualitatively different from ordinary recollections: they carry the original emotional and physiological intensity. They are not remembered — they are re-experienced. This is Criterion B — the re-experiencing cluster — and it is the most specific feature of PTSD.
You avoid everything associated with the trauma — and the avoidance expands over time. Not just thinking about what happened, but the places, people, conversations, activities, or situations that could bring it back. The avoidance starts as a protective strategy and progressively narrows your world. Many people with PTSD are not aware of how much their daily choices have reorganized around what they cannot approach. This is Criterion C — and the expanding avoidance is one of the most reliable signs that the condition is progressing rather than resolving.
Your beliefs about yourself, others, or the world changed permanently after the trauma. “The world is not safe.” “I am permanently damaged.” “I can’t trust anyone.” “It was my fault.” These are not fleeting thoughts — they are the persistent negative cognitions of Criterion D, embedded in how you interpret everything that follows the trauma. They are not character flaws or accurate assessments — they are the cognitive residue of the trauma itself, and they respond to treatment.
You feel emotionally numb or cut off from other people — even people you love. The emotional numbing and detachment of PTSD — the inability to feel positive emotions, the sense of being permanently separate from other people — is frequently misidentified as depression or introversion. It is the brain’s protective response to overwhelming emotional activation during trauma, which persists as a chronic state afterward.
You are constantly on guard — scanning for threats even when you are objectively safe. Hypervigilance is not anxiety about specific things — it is a pervasive, exhausting state of alert readiness that never fully switches off. The startle response is exaggerated. Ordinary sounds or movements produce a disproportionate physical response. You cannot completely relax, even in environments your rational mind recognizes as safe. This is Criterion E — the hyperarousal cluster — driven by a nervous system that was recalibrated by the trauma to treat the world as permanently dangerous.
Your sleep is disrupted by nightmares or by difficulty staying asleep. PTSD-related sleep disturbance is qualitatively different from ordinary insomnia. Nightmares related to the trauma — sometimes replaying the event, sometimes symbolically connected to it — disrupt sleep in ways that produce cumulative exhaustion and make the daytime symptoms more difficult to manage. Sleep disruption appears in both Criterion E (hyperarousal) and as a standalone functional impact.
The symptoms have been present for more than a month and are affecting your daily functioning. Criterion F (one-month duration) and Criterion G (functional impairment) are what distinguish PTSD from acute stress disorder or a normal grief and recovery response. If the symptoms have been consistently present for more than a month and are affecting your work, your relationships, or your ability to function in daily life — that pattern meets the chronicity and impairment criteria regardless of how long ago the trauma occurred.
PTSD vs C-PTSD vs Acute Stress Disorder vs Adjustment Disorder
| Feature | PTSD | Complex PTSD (C-PTSD) | Acute Stress Disorder | Adjustment Disorder |
|---|---|---|---|---|
| Diagnostic system | DSM-5-TR 309.81 AND ICD-11 | ICD-11 only — NOT in DSM-5-TR | DSM-5-TR 308.3 AND ICD-11 | DSM-5-TR 309.xx AND ICD-11 |
| Trauma type | Single or multiple events meeting Criterion A — actual or threatened death, serious injury, sexual violence | Prolonged, repeated, inescapable trauma — childhood abuse, domestic violence, torture, captivity | Same Criterion A events as PTSD | Any identifiable stressor — not required to meet Criterion A severity |
| Duration | More than 1 month (Criterion F) | Chronic — typically years; no specific duration criterion | 3 days to 1 month after trauma | Within 3 months of the stressor, it resolves within 6 months of the stressor ending |
| Additional features beyond PTSD | Core 4-cluster symptom profile (B, C, D, E) | PTSD symptoms PLUS disturbances in self-organization: affect dysregulation, negative self-concept, relational disturbances | Same symptom clusters as PTSD but shorter duration | Emotional or behavioral symptoms in response to a stressor do not require PTSD symptom clusters |
| Typical trauma history | Any Criterion A event — assault, accident, combat, disaster, medical trauma, witnessing | Childhood abuse, domestic violence, trafficking, prolonged captivity, repeated sexual abuse | Recent Criterion A event — symptoms are a normal acute response that hasn’t yet resolved | Divorce, job loss, illness, relationship problems — any significant stressor |
| PsyMed test | This test | This test (C-PTSD section below) | Anxiety Test | Depression Test |
What Is Complex PTSD (C-PTSD)?
Complex PTSD (C-PTSD) is recognized as a distinct diagnosis in the World Health Organization’s International Classification of Diseases, 11th Edition (ICD-11, 2022). It is not a separate diagnosis in the DSM-5-TR — this matters clinically because treatment approach, diagnostic formulation, and insurance coding differ depending on which framework your clinician uses.
C-PTSD typically develops following prolonged, repeated, or inescapable trauma — childhood physical or sexual abuse, domestic violence, torture, human trafficking, or prolonged captivity. The ICD-11 defines C-PTSD as having all the symptoms of PTSD plus three additional features collectively called disturbances in self-organization (DSO):
Affect dysregulation: Difficulty regulating emotional responses — intense, rapidly shifting emotions; chronic shame or guilt; emotional numbing that alternates with emotional flooding.
Negative self-concept: A stable, pervasive sense of being permanently damaged, worthless, or fundamentally different from other people — often experienced as a core identity rather than a temporary mood state.
Relational disturbances: Persistent difficulty sustaining relationships — either avoiding closeness, having chaotic or unstable relationships, or experiencing pervasive distrust of others.
C-PTSD is more commonly associated with early-life trauma (abuse, neglect, domestic violence) where the traumatic exposure occurred during critical developmental periods and was perpetrated by attachment figures. The resulting disturbances to self and relationship functioning go significantly beyond the four PTSD symptom clusters and require a different therapeutic approach — specifically, longer-term, phase-based trauma therapy that addresses the self-organization disturbances before trauma processing.
About This Test — The PCL-5 Framework
This PTSD Test is based on the PCL-5 (PTSD Checklist for DSM-5), developed by Dr. Frank W. Weathers, Dr. Brett T. Litz, Dr. Terence M. Keane, Dr. Paul A. Palmieri, Dr. Brian P. Marx, and Dr. Paula P. Schnurr (2013) at the National Center for PTSD, U.S. Department of Veterans Affairs. It is the most widely used and extensively validated self-report measure of PTSD symptoms in both clinical and research settings.
The PCL-5 covers all 20 DSM-5 PTSD symptoms across the four Criterion B–E clusters: Criterion B (re-experiencing, items 1–5), Criterion C (avoidance, items 6–7), Criterion D (negative alterations in cognition and mood, items 8–14), and Criterion E (hyperarousal, items 15–20). It uses a 5-point scale from 0 (Not at all) to 4 (Extremely), with a total score range of 0–80.
The VA National Center for PTSD identifies a cut score of 31–33 as indicative of probable PTSD across samples. A provisional PTSD diagnosis can be made by treating items rated ≥2 (Moderately) as endorsed and requiring at least one B item, one C item, two D items, and two E items (VA National Center for PTSD, 2013).
Answer each question based on how much you have been bothered by that problem in the past month. The past month time frame is the validated PCL-5 recall period.
- Not at all = 0
- A little bit = 1
- Moderately = 2
- Quite a bit = 3
- Extremely = 4
Total range: 0–80. This is a screening tool. Only a qualified mental health professional can diagnose PTSD.
Understanding Your PTSD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 20 | Low — Few PTSD Indicators | Responses suggest few significant PTSD symptoms at this time. Occasional distress related to difficult memories may be present without a pattern consistent with PTSD. |
| 21 – 40 | Mild — Some PTSD Symptoms Present | Some PTSD symptom patterns present. Scores in this range — particularly above 31 — are in the probable PTSD range per VA National Center for PTSD thresholds. Professional evaluation is recommended. |
| 41 – 60 | Moderate — Significant PTSD Symptoms | Significant PTSD symptom burden across multiple clusters. Consistent with moderate-to-severe PTSD. Professional evaluation and trauma-focused treatment are strongly recommended. |
| 61 – 80 | High — Severe PTSD Indicators | Severe PTSD symptom burden across most clusters. Professional evaluation and trauma-focused treatment are urgently recommended. Please reach out for support. |
Treatment for PTSD
PTSD is highly treatable. The following approaches have the strongest evidence base:
Prolonged Exposure (PE). Developed by Dr. Edna Foa at the University of Pennsylvania, PE is one of the two first-line trauma-focused treatments endorsed by the VA and the American Psychological Association. It involves gradual, systematic confrontation of trauma-related memories and avoided situations — reducing the fear response through extinction learning. PE typically produces significant symptom reduction in 8–15 sessions.
Cognitive Processing Therapy (CPT). The other primary first-line treatment for PTSD. CPT targets the maladaptive cognitions that maintain PTSD — particularly the stuck points around self-blame, trust, safety, power and control, esteem, and intimacy — through structured written and verbal processing exercises. Particularly effective for PTSD associated with sexual assault and military trauma.
EMDR (Eye Movement Desensitization and Reprocessing). Developed by Dr. Francine Shapiro, EMDR uses bilateral stimulation (eye movements, tapping, or auditory tones) while processing traumatic memories — facilitating the integration and re-encoding of traumatic material. Equally effective as PE and CPT in meta-analyses.
Pharmacotherapy. Sertraline and paroxetine are FDA-approved for PTSD and have the strongest evidence base among medications. They are used both as a standalone treatment and to support engagement with trauma-focused therapy by reducing baseline anxiety and intrusive symptom intensity.
For C-PTSD specifically: Phase-based treatment is the standard of care — stabilization (skills for emotional regulation, distress tolerance, and grounding) before trauma processing. Schema Therapy and Dialectical Behavior Therapy (DBT) are frequently used in the stabilization phase for people with significant affect dysregulation and self-organization disturbances.
Frequently Asked Questions
What is PTSD?
Post-Traumatic Stress Disorder (PTSD) is a Trauma- and Stressor-Related Disorder (DSM-5-TR 309.81 / F43.10) that can develop after exposure to actual or threatened death, serious injury, or sexual violence. It is characterized by four symptom clusters: re-experiencing (flashbacks, nightmares, intrusive memories), avoidance, negative alterations in cognition and mood, and hyperarousal. Approximately 6% of U.S. adults will experience PTSD in their lifetime, and around 5% (~13 million Americans) are affected in any given year. Women are twice as likely as men to develop PTSD (National Center for PTSD, 2024).
What is the difference between PTSD and C-PTSD?
Complex PTSD (C-PTSD) is recognized as a distinct diagnosis in the ICD-11 (2022) but is not a separate diagnosis in the DSM-5-TR. PTSD involves the four core symptom clusters (re-experiencing, avoidance, negative cognition/mood, hyperarousal). C-PTSD includes all PTSD symptoms plus three additional disturbances in self-organization: affect dysregulation, a persistently negative self-concept, and relational disturbances. C-PTSD typically develops after prolonged, repeated, inescapable trauma — childhood abuse, domestic violence, torture — rather than a single traumatic event. Treatment for C-PTSD typically uses a phase-based approach: stabilization before trauma processing.
What is the PCL-5?
The PCL-5 (PTSD Checklist for DSM-5) is a 20-item self-report measure developed by Weathers, Litz, Keane, Palmieri, Marx, and Schnurr (2013) at the National Center for PTSD, U.S. Department of Veterans Affairs. It assesses all 20 DSM-5 PTSD symptoms across the four Criterion B–E clusters using a 0–4 scale (Not at all to Extremely), with a total score range of 0–80. It is the most widely used validated self-report PTSD measure in clinical and research settings. The VA National Center for PTSD identifies a cut score of 31–33 as indicative of probable PTSD across samples.
What are the most effective treatments for PTSD?
The two first-line treatments with the strongest evidence base, endorsed by both the VA and the American Psychological Association, are Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT). EMDR (Eye Movement Desensitization and Reprocessing) is equally effective in meta-analyses. Sertraline and paroxetine are the FDA-approved medications for PTSD. For C-PTSD, phase-based treatment is standard — stabilization before trauma processing. All three first-line treatments produce large treatment effects and lasting symptom reduction in the majority of people who complete them.
Can PTSD develop from childhood trauma?
Yes — childhood trauma, including physical abuse, sexual abuse, emotional abuse, neglect, exposure to domestic violence, and community violence, can all produce PTSD. When childhood trauma is prolonged, repeated, and perpetrated by caregivers or attachment figures, the resulting presentation often meets criteria for C-PTSD (ICD-11) rather than standard PTSD — with the additional self-organization disturbances reflecting the developmental impact of chronic early trauma on identity formation, affect regulation, and the capacity for relationships. The Dissociation Test may also be relevant where childhood trauma involved significant dissociation.
How is PTSD different from anxiety or depression?
PTSD shares features with both anxiety disorders (hyperarousal, avoidance) and depression (negative mood, anhedonia, detachment) — which is one reason it is frequently misdiagnosed as one or the other. The distinguishing feature of PTSD is its etiological specificity: it requires a Criterion A traumatic event, and its symptoms are organized around that event — the re-experiencing symptoms are specifically trauma-linked, the avoidance is specifically of trauma reminders, and the negative cognitions are specifically shaped by the trauma and its meaning. Treatment differs as well: trauma-focused therapy (PE, CPT, EMDR) is more effective for PTSD than standard anxiety or depression treatment.
Is PTSD a sign of weakness?
No. PTSD is not a sign of weakness, lack of resilience, or personal failure. It is a neurobiological response to overwhelming experience — a failure of the brain’s normal trauma processing to consolidate the traumatic memory into narrative storage rather than keeping it in its original sensory, arousal-linked form. Research consistently shows that PTSD is influenced by biological factors (neurobiological vulnerability, prior trauma history, genetic factors) as much as by psychological ones — and that many people who develop PTSD had previously coped well with significant adversity. The stigma around PTSD — particularly in military and first-responder contexts — is one of the main barriers to treatment-seeking. PTSD is a recognized medical condition with effective treatments, not a character failing.
Related Tests
- Anxiety Test — PTSD shares hyperarousal and avoidance features with anxiety disorders; generalized anxiety is among the most common PTSD comorbidities
- Clinical Depression Test — depression is the most common PTSD comorbidity; the negative cognition and mood cluster of PTSD overlaps significantly with depressive presentations
- Dissociation Test — dissociative symptoms are common in PTSD, particularly where childhood trauma or extreme trauma is involved; DID can develop from severe, chronic early trauma
- Suicidal Ideation Test — PTSD carries elevated suicide risk; please assess if thoughts of self-harm have been present alongside these symptoms
- Borderline Personality Disorder Test — BPD and C-PTSD share significant surface features (affect dysregulation, relational instability, self-harm) and are frequently confused or co-occurring
- Burnout Test — occupational trauma and secondary traumatic stress can produce PTSD-like presentations; worth assessing for first responders and healthcare workers
- Agoraphobia Test — PTSD-related avoidance can extend to produce agoraphobic patterns; both involve avoidance driven by fear of specific triggering situations
- Social Anxiety Test — interpersonal trauma (assault, abuse) frequently produces social anxiety alongside PTSD
- ADHD Test — PTSD concentration difficulties and hyperarousal can closely mimic ADHD; the two frequently co-occur and can be difficult to distinguish
- Anhedonia Test — loss of interest and inability to experience positive emotions is a core PTSD feature worth assessing separately
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Post-Traumatic Stress Disorder 309.81 (F43.10). psychiatry.org
- Weathers, F.W., Litz, B.T., Keane, T.M., Palmieri, P.A., Marx, B.P., & Schnurr, P.P. (2013). The PTSD Checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD at www.ptsd.va.gov. ptsd.va.gov
- National Center for PTSD, U.S. Department of Veterans Affairs. (2024). How Common is PTSD in Adults? ptsd.va.gov
- World Health Organization. (2024). Post-traumatic stress disorder. WHO Fact Sheet. who.int
- Kessler, R.C., Aguilar-Gaxiola, S., Alonso, J., et al. (2017). Trauma and PTSD in the WHO World Mental Health Surveys. European Journal of Psychotraumatology, 8(Suppl 5), 1353383. [Sexual assault — highest conditional PTSD risk] doi.org/10.1080/20008198.2017.1353383
- Blevins, C.A., Weathers, F.W., Davis, M.T., Witte, T.K., & Domino, J.L. (2015). The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress, 28(6), 489–498. doi.org/10.1002/jts.22059
- World Health Organization. (2022). International Classification of Diseases, 11th Revision (ICD-11). Complex post-traumatic stress disorder. icd.who.int
- Foa, E.B., Hembree, E.A., Rothbaum, B.O., & Rauch, S.A.M. (2019). Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences (2nd ed.). Oxford University Press.
- Resick, P.A., Monson, C.M., & Chard, K.M. (2017). Cognitive Processing Therapy for PTSD: A Comprehensive Manual. Guilford Press.
- Wikipedia. (2025). Post-traumatic stress disorder. en.wikipedia.org