
Most people feel nervous before a job interview, a first date, or a public presentation. That kind of situational anxiety is normal — it fades once the situation passes. But for millions of people, social anxiety goes far deeper. The fear of being judged, embarrassed, or humiliated in social situations is so intense and persistent that it shapes every decision — which events to avoid, which relationships to forgo, which opportunities to let pass quietly. The anxiety doesn’t fade with the situation. It grows with every avoidance.
Social Anxiety Disorder is the third most common mental health disorder in the world, after depression and alcohol use disorder, affecting approximately 15 million US adults — around 7.1% of the population (ADAA, 2022). Yet the average person with social anxiety waits over ten years before seeking help, often believing that the fear is simply who they are rather than a clinically recognized, highly treatable condition (ADAA, 2022).
This free Social Anxiety Test covers all DSM-5-TR diagnostic criteria for Social Anxiety Disorder (APA, 2022), inspired by the Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987) and the Social Phobia Inventory (SPIN; Connor et al., 2000) — the two most widely used clinical screening instruments for Social Anxiety Disorder (SAD). 15 questions. Based on the past 6 months. Instant, private results.
What Is Social Anxiety Disorder?
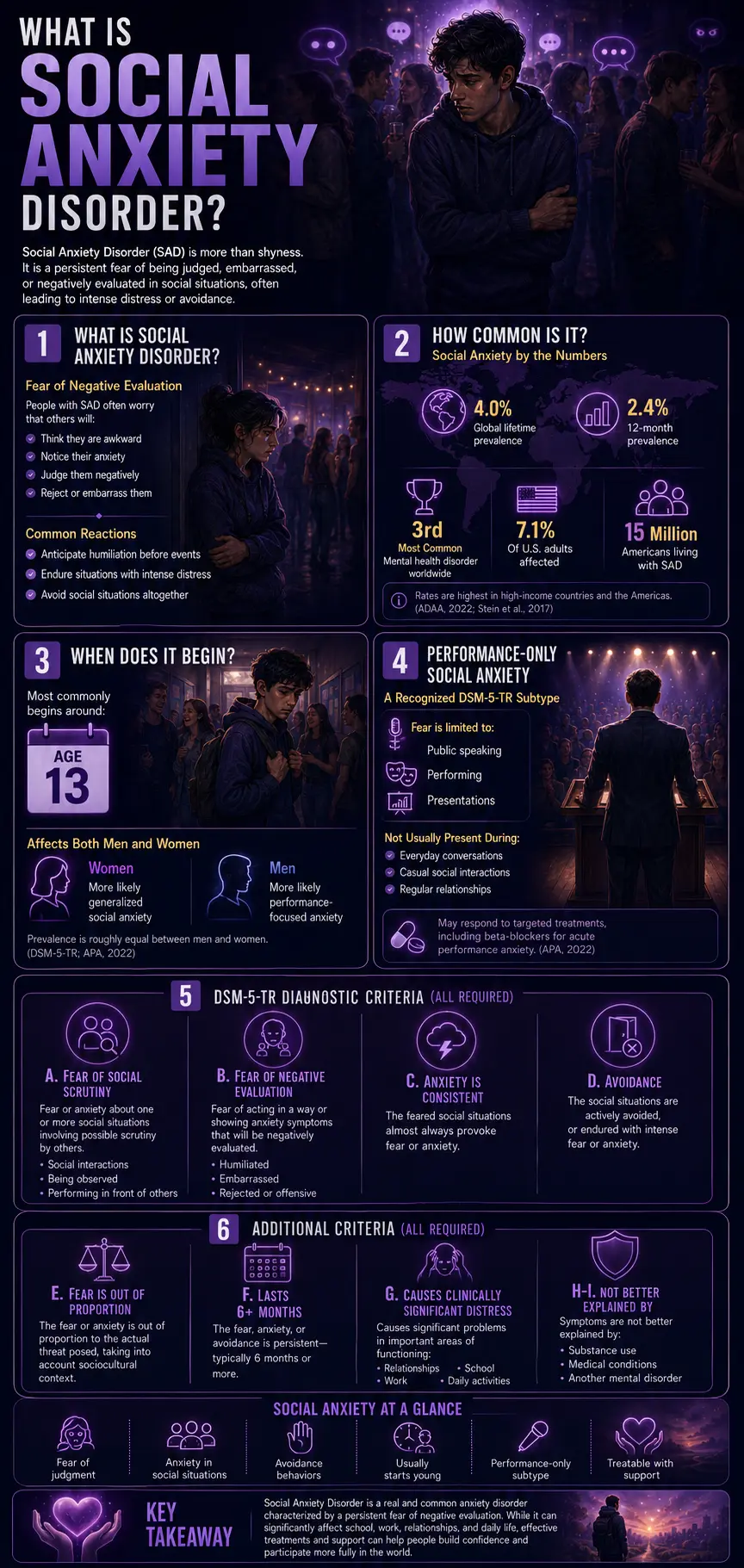
Social Anxiety Disorder (SAD) — DSM-5-TR code 300.23 (F40.10), formerly listed parenthetically as “social phobia” in earlier DSM editions — is an anxiety disorder characterized by marked, persistent fear or anxiety about social or performance situations in which a person may be exposed to scrutiny by others. The fear is specifically about being negatively evaluated: being judged as incompetent, awkward, embarrassing, or offensive. People with SAD anticipate humiliation before social situations, endure them with intense distress, or avoid them altogether (APA, 2022).
SAD is the third most common mental health disorder worldwide, after depression and alcohol use disorder (ADAA, 2022). Global lifetime prevalence is 4.0%, and 12-month prevalence is 2.4%, based on the World Mental Health Survey Initiative covering 28 countries and 142,405 respondents (Stein et al., 2017, Psychological Medicine). Rates are consistently higher in high-income countries and the Americas. In the United States, approximately 7.1% of adults — around 15 million people — are affected (ADAA, 2022). Onset is typically early: the disorder most commonly begins around age 13. Prevalence is roughly equal between men and women, though women are more likely to present with generalized social anxiety, while men are more likely to present with performance-specific fear (DSM-5-TR; APA, 2022).
The DSM-5-TR recognizes a “performance-only” specifier for cases in which the fear is limited exclusively to speaking or performing in public — not to general social interaction. This subtype has a somewhat different profile and may respond to specific targeted interventions, including beta-blockers for acute performance anxiety (APA, 2022).
The full DSM-5-TR diagnostic criteria for SAD (all of the following required; APA, 2022):
- Criterion A: Marked fear or anxiety about one or more social situations in which the person may be exposed to possible scrutiny by others — social interactions, being observed, performing in front of others.
- Criterion B: The person fears that they will act in a way or show anxiety symptoms that will be negatively evaluated — humiliated, embarrassed, rejected, or offensive to others.
- Criterion C: The feared social situations almost always provoke fear or anxiety.
- Criterion D: The social situations are actively avoided or endured with intense fear or anxiety.
- Criterion E: The fear or anxiety is out of proportion to the actual threat posed, taking into account sociocultural context.
- Criterion F: The fear, anxiety, or avoidance is persistent — typically 6 months or more.
- Criterion G: Causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- Criteria H–I: Not better explained by substances, a medical condition, or another mental disorder.
Signs You Might Have Social Anxiety Disorder
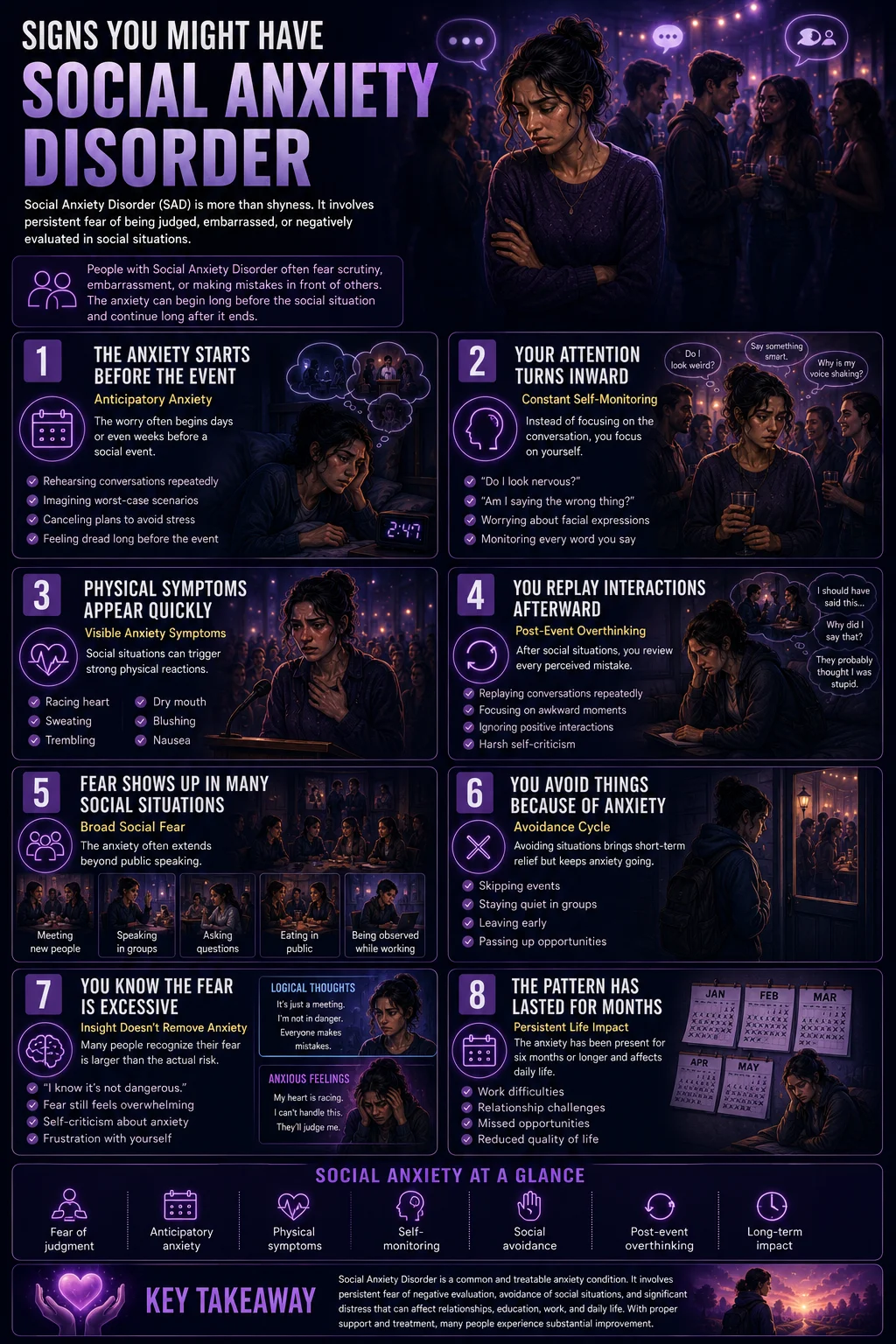
Social anxiety is among the most commonly misidentified conditions — both by people who have it (who attribute it to shyness or introversion) and by clinicians who may not probe sufficiently to distinguish normal social discomfort from the clinical pattern. These are the signs that most consistently indicate SAD may be present.
The anticipatory anxiety is often worse than the situation itself. Days or weeks before a social event, the dread arrives. Mental rehearsal of worst-case scenarios: saying the wrong thing, going blank, visibly shaking, being judged. The anxiety before is intense enough that many people cancel plans simply to relieve it — which provides immediate relief and reinforces the avoidance cycle. This anticipatory pattern, extending well beyond the situation itself, is one of the most clinically specific features of SAD. Normal situational nervousness doesn’t begin a week in advance.
In social situations, your attention turns sharply inward. Instead of focusing on the conversation or the event, a significant portion of your cognitive resources is consumed by self-monitoring: how am I coming across? Do I look nervous? Is my voice shaking? Am I saying the right things? This self-focused attention is both a symptom and a maintenance mechanism — it consumes the attentional resources needed to actually engage with the social situation, making the social anxiety worse and the interaction more awkward.
Physical symptoms appear reliably in feared social situations. Blushing, sweating, trembling, racing heart, nausea, voice shaking, dry mouth. These symptoms are distressing in themselves, but for people with Social Anxiety Disorder (SAD) they are particularly problematic because they fear others will notice them — creating a secondary fear of the visible symptoms of anxiety on top of the primary fear of negative evaluation. The physiological symptoms themselves become part of what is feared.
You replay social situations afterward — and the replay is harsh. After a social event, the post-event processing begins: a detailed review of every perceived mistake, embarrassing moment, or wrong thing said. The review is systematically distorted — negatives are amplified and made central, positives are dismissed or minimized as flukes. This post-event processing maintains SAD by reinforcing negative beliefs about social performance and making the next similar situation feel even more threatening. It is a cognitive maintenance mechanism that keeps the disorder active even when no social situation is currently happening.
The fear extends across multiple social situation types. SAD is not specifically public speaking fear (though that is common) — it extends across the five LSAS factor domains: speaking or performing in public; eating or drinking in front of others; assertive behaviors (disagreeing, returning items, asking questions); working or writing while being observed; and interactions with strangers or unfamiliar people. The generalized subtype of SAD involves fear across most or all of these domains; the performance-only specifier covers only the public speaking/performance domain. If the fear is broad and extends across most social contexts, that breadth is diagnostically significant.
You avoid situations or activities specifically because of social anxiety. Job opportunities, social events, romantic possibilities, classes, or professional situations that would require being in a feared situation. The avoidance may be obvious (not going to parties) or subtle (attending but staying on the periphery, not contributing to conversations, leaving early). DSM-5-TR Criterion D — active avoidance or endurance with intense distress — is met either way. The avoidance is relief-seeking behavior that maintains the disorder by preventing the disconfirming experience of tolerating anxiety until it naturally decreases.
The fear is out of proportion to the actual threat — and you know it. DSM-5-TR Criterion E requires that the fear or anxiety be out of proportion to actual danger. Many people with SAD have the meta-awareness that their fear is excessive — “I know rationally that speaking in this meeting is not dangerous, but I feel as if it is.” This awareness does not reduce the fear. It adds a layer of self-criticism (why can’t I just be normal?) that can compound the distress.
The pattern has been present for at least six months and is affecting your life. Criterion F (6-month duration) and Criterion G (functional impairment) together distinguish SAD from a temporary anxious period. If the social fear has been consistently present for more than six months and is meaningfully affecting your work, relationships, or daily life — that chronicity and impairment are diagnostically significant regardless of how long ago the pattern began.
Social Anxiety vs Shyness vs Agoraphobia vs AVPD
| Feature | Social Anxiety Disorder (SAD) | Shyness (Trait) | Agoraphobia | Avoidant PD (AVPD) |
|---|---|---|---|---|
| Core fear | Negative evaluation — being judged as embarrassing, incompetent, or offensive | Social discomfort — not a fear of evaluation per se, but inhibition in unfamiliar contexts | Being in situations where escape is difficult or help is unavailable — not about judgment | Inadequacy and negative evaluation — same as SAD but more pervasive and identity-level |
| Functional impairment | Required for diagnosis — clinically significant distress or impairment (Criterion G) | Not required — shy people typically function well without clinically significant impairment | Required — avoidance restricts mobility and daily independence | Required — pervasive avoidance affects work and relationships across domains |
| Does anxiety ease with familiarity? | Often yes — people with SAD may feel relatively comfortable with close friends; the fear is typically context-specific | Yes — shyness typically reduces substantially as situations become familiar | Not primarily about familiarity — the fear is about the situation’s escape properties, not the people in it | Partially — AVPD involves pervasive interpersonal inadequacy that doesn’t ease fully even in long-standing relationships |
| Companion effect | Having a trusted companion may ease anxiety in social situations, but it is not a required feature | Often helps — social support reduces inhibition | A trusted companion specifically enables entry into avoided situations — this is a diagnostic feature of agoraphobia | Companions help less than in SAD — the feelings of inadequacy are more pervasive and internal |
| DSM-5-TR classification | Anxiety disorder — 300.23 (F40.10) | Not a disorder — normal personality trait | Anxiety disorder — 300.22 (F40.00) | Cluster C personality disorder — 301.82 (F60.6) |
| Duration criterion | 6+ months (Criterion F) | No criterion — trait, not disorder | 6+ months (DSM-5-TR) | Since early adulthood — pervasive, lifelong pattern |
| PsyMed test | This test | N/A | Agoraphobia Test | Avoidant PD Test |
The SAD/AVPD distinction deserves particular attention. They share the same core fear (negative evaluation) and produce similar behavioral avoidance — which is why many clinicians and patients cannot distinguish them from surface presentation alone. The critical differences: SAD is an anxiety disorder (episodic, situation-specific, typically responsive to CBT in 12–16 sessions); AVPD is a personality disorder (pervasive, identity-level, requiring longer-term schema-focused or psychodynamic work). SAD and AVPD frequently co-occur — estimates range from 25–89% comorbidity, depending on criteria (DSM-5-TR notes they may represent different expressions of the same underlying vulnerability). If the avoidance feels less like situational anxiety and more like a core defining feature of who you are — present across virtually all relationships and contexts since early adulthood — the Avoidant Personality Disorder Test is worth completing alongside this one.
What Causes Social Anxiety Disorder?
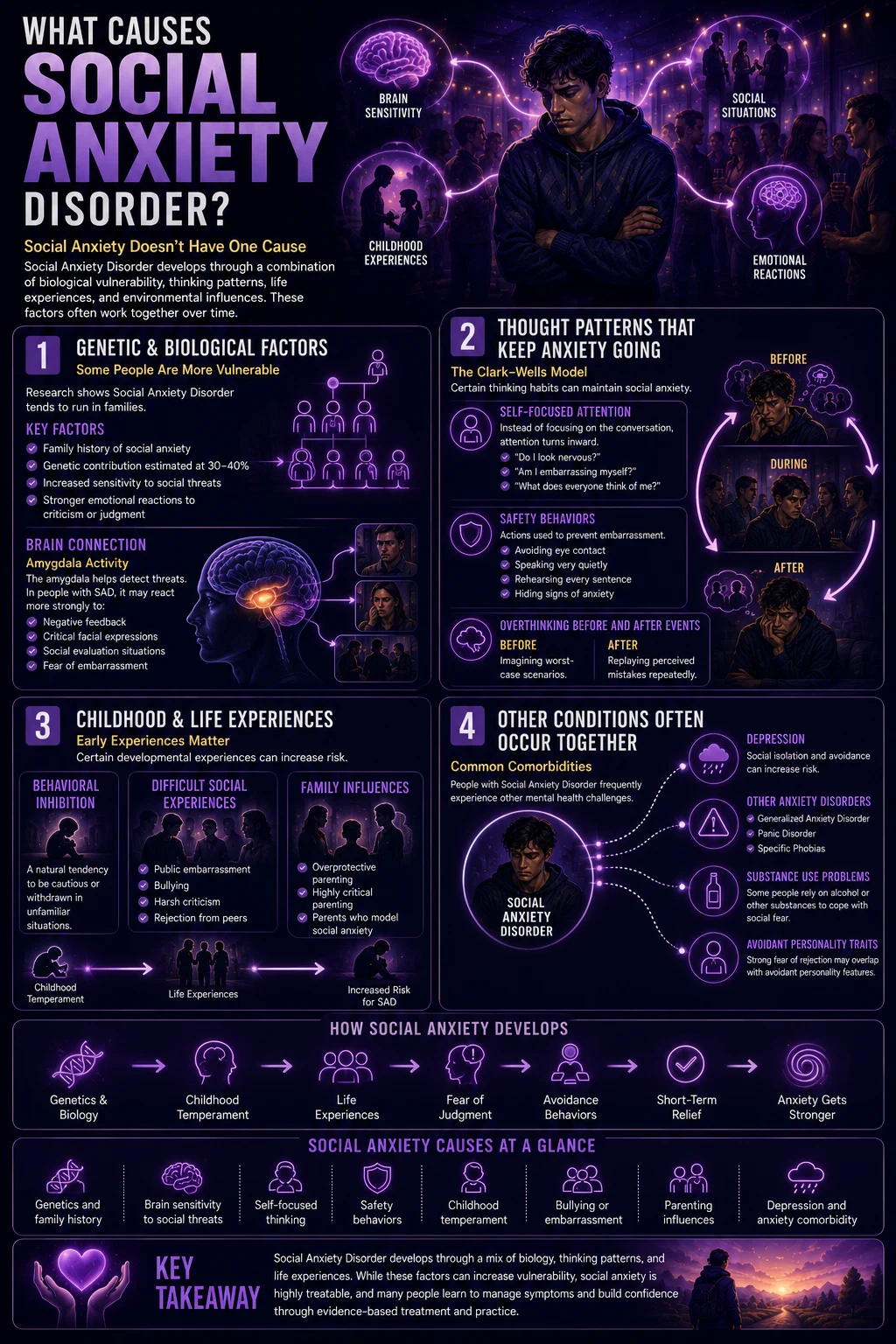
SAD etiology is well characterized, involving the interaction among biological vulnerability, cognitive patterns, and developmental experience.
Genetic and biological factors. SAD has significant heritability — estimated at 30–40% in twin studies. First-degree relatives of people with SAD have higher rates of the disorder. Neurobiologically, the amygdala — the brain’s threat-detection center — shows heightened reactivity to social threat cues in people with SAD, including faces, social scenarios, and negative evaluation feedback. The serotonergic and dopaminergic systems are implicated, which aligns with the pharmacological response to SSRIs (first-line pharmacotherapy for SAD).
Cognitive maintaining factors. The most influential cognitive model of SAD was developed by David M. Clark and Adrian Wells (1995, Behaviour Research and Therapy) and subsequently refined by Clark (1999, 2001). The Clark-Wells model identifies the key maintaining mechanisms: (1) self-focused attention that depletes resources for social engagement; (2) the use of “safety behaviors” — subtle actions to prevent feared outcomes (holding a cup tightly to prevent visible shaking, avoiding eye contact to prevent humiliation) — that paradoxically maintain anxiety by preventing disconfirmation; (3) anticipatory anxiety and post-event processing that contaminate memory and expectations of future situations.
Developmental and behavioral factors. Behavioral inhibition in childhood — a temperamental tendency to withdraw from novel or unfamiliar stimuli — is one of the strongest developmental predictors of SAD. Specific learning experiences (public humiliation, being the target of bullying, embarrassing incidents in front of groups) can precipitate or intensify SAD. Parenting styles involving criticism, overprotection, or modeling of social anxiety also contribute.
Comorbidities. SAD has very high comorbidity rates. Major depressive disorder is the most common comorbidity — the social isolation and functional impairment of SAD predictably produce depression over time. Other anxiety disorders commonly co-occur, as do substance use disorders (alcohol is frequently used as a social anxiety management strategy). Avoidant Personality Disorder is the most common personality disorder comorbidity.
About This Test — LSAS and SPIN Framework
This Social Anxiety Test is inspired by the two most widely used clinical screening instruments for SAD:
The Liebowitz Social Anxiety Scale (LSAS), introduced by Dr. Michael R. Liebowitz in 1987, is the most frequently used measure of social anxiety in research, clinical, and pharmacotherapy studies. The LSAS assesses both fear and avoidance across 24 social and performance situations — providing a comprehensive profile of the two key behavioral dimensions of SAD. A large-scale cross-cultural study (N=31,243; PMC, 2019) validated a 5-factor structure of the LSAS: (1) speaking in public, (2) eating/drinking in front of others, (3) assertive behaviors, (4) working/writing while observed, and (5) interactions with strangers. All five factors are covered in this test.
The Social Phobia Inventory (SPIN), developed by Connor and colleagues (2000, British Journal of Psychiatry), is a 17-item self-report instrument that assesses fear, avoidance, and physiological symptoms of social anxiety. A SPIN score of 19 or above is considered indicative of probable SAD in clinical settings.
Answer based on your consistent experience over the past 6 months — the recurring pattern across different social situations, not your best or worst individual experiences.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Total range: 0–60. This is a screening tool. Only a qualified mental health professional can diagnose Social Anxiety Disorder through a comprehensive clinical assessment.
Understanding Your Social Anxiety Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Social Anxiety Indicators | Social anxiety patterns are not significantly present. Normal social discomfort may be present without a pattern consistent with Social Anxiety Disorder. |
| 16 – 30 | Mild — Some Social Anxiety Patterns | Some social anxiety features are present across one or more domains. Consistent with subthreshold SAD or non-generalized social anxiety. Worth professional discussion. |
| 31 – 45 | Moderate — Significant Social Anxiety | Significant social anxiety across multiple domains. Consistent with generalized SAD. Professional evaluation and CBT-based treatment are recommended. |
| 46 – 60 | High — Strong Social Anxiety Indicators | Pervasive and severe social anxiety across most domains. Consistent with severe generalized SAD. Professional evaluation and treatment are urgently recommended. |
Evidence-Based Treatment for Social Anxiety Disorder
SAD is highly treatable. Four major international clinical guidelines — NICE (UK, 2024), the American Psychological Association, the World Federation of Societies of Biological Psychiatry (WFSBP), and the British Association for Psychopharmacology — all recommend CBT as the first-line treatment for SAD in adults.
Cognitive Behavioral Therapy (CBT) — gold standard. CBT for SAD typically involves 12–16 weekly sessions and is structured around the Clark-Wells model: identifying and modifying the self-focused attention and safety behaviors that maintain social anxiety; video feedback to correct the distorted self-image that drives the fear of appearing visibly anxious; behavioral experiments that test specific predictions about feared social outcomes; and graduated exposure to feared situations with safety behaviors removed. Effect sizes are large, and outcomes are maintained at long-term follow-up (Clark et al., 1999, 2001; Liebowitz et al., 2002).
Pharmacotherapy — SSRIs and SNRIs. First-line medications: sertraline, paroxetine, escitalopram (SSRIs), and venlafaxine (SNRI) all have strong evidence for SAD. MAOIs (phenelzine) have the longest evidence history but are rarely first-line due to dietary restrictions. Benzodiazepines provide short-term relief but are not recommended long-term due to dependence risk and interference with the extinction learning that CBT produces. Beta-blockers (propranolol) are sometimes used for the “performance only” specifier — reducing the physiological symptoms in specific performance contexts without treating the underlying disorder.
Group CBT. Group-delivered CBT is specifically effective for SAD because the group setting provides an in-session exposure context — the experience of interacting with other group members while using less self-monitoring and fewer safety behaviors is itself therapeutic. Group CBT is widely available and often more accessible than individual therapy.
NICE-endorsed stepped care. NICE (2024) recommends a stepped approach: Step 1 involves psychoeducation and self-help resources; Step 2 involves low-intensity guided self-help (CBT-based workbooks or computerized CBT with support); Step 3 involves CBT or a CBT-based group program; Step 4 involves combined CBT and medication for complex or treatment-resistant presentations.
Frequently Asked Questions
What is Social Anxiety Disorder?
Social Anxiety Disorder (SAD; DSM-5-TR 300.23 / F40.10) is an anxiety disorder characterized by marked, persistent fear or anxiety about social or performance situations in which a person may be exposed to scrutiny and negatively evaluated. All of the following must be present: marked fear in social situations (Criterion A); fear of negative evaluation (B); almost always provoked (C); active avoidance or endurance with intense distress (D); disproportionate fear (E); duration 6+ months (F); significant distress or impairment (G). SAD is the third most common mental health disorder worldwide, affecting approximately 15 million US adults (7.1%). Onset is typically around age 13. CBT is the gold-standard treatment (NICE 2024; APA; WFSBP).
What is the difference between social anxiety and shyness?
Shyness is a personality trait — a tendency toward social inhibition in unfamiliar or novel contexts that does not cause clinically significant impairment. Most shy people function well, feel comfortable with familiar people, and do not experience the persistent anticipatory anxiety, self-focused attention, physical symptoms, and avoidance that characterize SAD. Social Anxiety Disorder involves all of these features — intense, persistent fear of negative evaluation across social situations, accompanied by avoidance that meaningfully restricts daily life, for at least 6 months. Many people with SAD are not shy in the traditional sense — they may appear socially competent while experiencing significant internal distress. The distinction matters because shyness does not require treatment; SAD does, and it responds well to it.
What are the most common situations feared in social anxiety?
The LSAS 5-factor structure (PMC, 2019) identifies: (1) speaking or performing in public; (2) eating or drinking in front of others; (3) assertive behaviors (disagreeing, complaining, returning items); (4) working or writing while being observed; and (5) interactions with strangers. Beyond these core domains, other commonly feared situations include: starting or maintaining conversations, meeting new people, attending parties or gatherings, being the center of attention, speaking up in meetings or classes, using public restrooms when others are present, making phone calls to strangers, dating, and asserting oneself or disagreeing with others. The “performance only” DSM-5-TR specifier applies when the fear is exclusively limited to speaking or performing in public — not general social interaction.
Is social anxiety disorder treatable?
Yes — SAD is one of the most treatable anxiety disorders. CBT specifically designed for SAD produces response rates of 70–80% in clinical trials, with large treatment effects that are maintained at long-term follow-up. The Clark-Wells CBT protocol — involving video feedback, attention retraining, behavioral experiments targeting safety behaviors, and graduated exposure — is the most extensively validated psychological treatment. SSRIs and SNRIs (sertraline, paroxetine, escitalopram, venlafaxine) are effective first-line medications. Combined CBT and pharmacotherapy is recommended for severe presentations (NICE 2024). The critical barrier to treatment is the average 10-year delay in seeking help — most people with SAD believe it is simply their personality rather than a treatable clinical condition.
What is the LSAS?
The Liebowitz Social Anxiety Scale (LSAS) was introduced by Dr. Michael R. Liebowitz in 1987 and is the most frequently used measure of social anxiety in research, clinical, and pharmacotherapy studies. The LSAS assesses both fear and avoidance across 24 social and performance situations (maximum total score: 144). Clinical cut-off points: scores below 30 suggest SAD is unlikely; 30–60 suggest possible non-generalized SAD; 60–90 suggest generalized SAD is very probable; scores above 90 indicate severe SAD (Mennin et al., cited in Wikipedia LSAS article). A 5-factor structure of the LSAS — speaking in public, eating/drinking in front of others, assertive behaviors, working/writing while observed, and interactions with strangers — was validated in a large cross-cultural study of 31,243 participants (PMC, 2019).
What is the difference between social anxiety and agoraphobia?
Social Anxiety Disorder and agoraphobia both involve fear of certain public situations and can produce overlapping avoidance behaviors. The critical distinction is the core fear: in SAD, the fear is about being negatively evaluated — being judged, embarrassed, or humiliated by others. In agoraphobia, the fear is about being in situations where escape might be difficult or help unavailable — the concern is about being trapped or incapacitated without rescue, not about social judgment. The presence of a trusted companion specifically enables entry into avoided situations in agoraphobia (a diagnostic feature) but does not necessarily do the same in SAD. The Agoraphobia Test covers the agoraphobia presentation specifically.
How does social anxiety relate to avoidant personality disorder?
SAD and Avoidant Personality Disorder (AVPD) share the same core fear — negative evaluation and social rejection — and produce very similar behavioral avoidance patterns. The primary distinctions: SAD is an anxiety disorder (episodic, situation-specific, typically responsive to CBT in 12–16 sessions); AVPD is a personality disorder (pervasive since early adulthood, identity-level, requiring longer-term therapeutic work). Comorbidity is high — estimates range from 25–89% depending on the criteria used. When both are present, treatment typically targets SAD symptoms first (with CBT) before addressing the broader AVPD character patterns (with Schema Therapy or psychodynamic approaches). The Avoidant Personality Disorder Test specifically covers the AVPD presentation.
Related Tests
- Anxiety Test — generalized anxiety disorder and social anxiety frequently co-occur; GAD involves worry across multiple life domains, not specifically social evaluation
- Avoidant Personality Disorder Test — the most important companion test; AVPD shares SAD’s core fear of negative evaluation but at a pervasive, personality-level intensity beginning in early adulthood
- Agoraphobia Test — agoraphobia and SAD both produce public-situation avoidance through fundamentally different fear mechanisms; important differential
- Scopophobia Test — fear of being watched or stared at specifically; can exist independently or as part of broader social anxiety
- Clinical Depression Test — depression is the most common social anxiety comorbidity; the social isolation and functional impairment of SAD frequently produce depressive episodes over time
- Burnout Test — the chronic effort required to manage and mask social anxiety in daily life is depleting; burnout and social anxiety frequently co-occur
- Imposter Syndrome Test — imposter syndrome and social anxiety share the fear of being exposed as inadequate; they co-occur and reinforce each other in performance and workplace contexts
- Schizotypal Personality Disorder Test — STPD involves social anxiety that does not ease with familiarity and is rooted in paranoid fears rather than evaluation concerns; important differential for persistent social withdrawal
- PTSD Test — interpersonal trauma can produce social anxiety symptoms; PTSD involving social situations should be distinguished from primary SAD
- NPC Test — conformity and social anxiety frequently co-occur; fear of standing out drives social conformity in anxious individuals
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Social Anxiety Disorder 300.23 (F40.10). psychiatry.org
- Stein, D.J., Lim, C.C.W., Roest, A.M., et al. (2017). The cross-national epidemiology of social anxiety disorder: Data from the World Mental Health Survey Initiative. Psychological Medicine, 47(14), 2534–2553. [4.0% lifetime; 2.4% 12-month; 28 countries; N=142,405] doi.org
- Liebowitz, M.R. (1987). Social phobia. Modern Problems of Pharmacopsychiatry, 22, 141–173. [LSAS development; 24 items; fear + avoidance]
- Connor, K.M., Davidson, J.R., Churchill, L.E., et al. (2000). Psychometric properties of the Social Phobia Inventory (SPIN). British Journal of Psychiatry, 176, 379–386. [SPIN development; 17 items; cut-off 19] doi.org
- Clark, D.M., & Wells, A. (1995). A cognitive model of social phobia. In R.G. Heimberg et al. (Eds.), Social Phobia: Diagnosis, Assessment, and Treatment. Guilford Press. [Clark-Wells model; self-focused attention; safety behaviors; anticipatory and post-event processing]
- Osório, F.L., Crippa, J.A.S., Loureiro, S.R., et al. (2019). Psychometric properties of the Liebowitz Social Anxiety Scale in a large cross-cultural Spanish and Portuguese-speaking sample. European Archives of Psychiatry and Clinical Neuroscience. PMC6781681. [5-factor structure; N=31,243] pmc.ncbi.nlm.nih.gov
- Anxiety and Depression Association of America. (2022). Social Anxiety Disorder. [15 million US adults; 7.1%; age 13 onset; 10-year treatment delay] adaa.org
- NICE. (2024). Social anxiety disorder: recognition, assessment and treatment. Clinical guideline [CG159]. [CBT first-line; stepped care; CCBT options] nice.org.uk
- Wikipedia. (2025). Liebowitz Social Anxiety Scale. [LSAS cut-off points; scoring thresholds] en.wikipedia.org
- Wikipedia. (2025). Social anxiety disorder. en.wikipedia.org