The highs don’t feel like crisis. They feel like yourself — but turned up. More energy than usual, less need for sleep, faster thinking, more confidence, a pull toward activity and connection that feels good even if it doesn’t quite make sense. And then it shifts. The low that follows isn’t depression exactly — it’s more like deflation. A flatness. A tiredness. A pulling back from the world that lasts until, at some point, it doesn’t.
And then it cycles again.
This is the lived experience of cyclothymia — a chronic mood cycling pattern that doesn’t reach the severity of bipolar I or II disorder, but doesn’t resolve either. The highs never become full manic or hypomanic episodes by clinical criteria. The lows never meet the threshold for major depressive episodes. But the pattern is always there — two years or more, barely any symptom-free stretches, the same cycling between elevated and depressed mood that affects relationships, work, self-perception, and the basic continuity of daily life.
This free Cyclothymia Test screens for Cyclothymic Disorder using DSM-5-TR diagnostic criteria (APA, 2022) across both mood poles — hypomanic and depressive symptom periods — as well as the cycling pattern, chronicity, and functional impact. 15 questions. Based on your experience over the past 2 years. Results are instant and private.
What Is Cyclothymia?
Cyclothymic Disorder — formally classified under DSM-5-TR code 301.13 (ICD-10: F34.0) — is a bipolar spectrum mood disorder characterized by recurrent periods of hypomanic symptoms and depressive symptoms that persist over a minimum of two years in adults (one year in children and adolescents), with no symptom-free interval exceeding two months at a time.
The critical defining feature is that neither mood pole reaches the full diagnostic threshold: the hypomanic periods do not meet full criteria for a hypomanic or manic episode, and the depressive periods do not meet full criteria for a major depressive episode. This subthreshold cycling — often described as “bipolar lite” or informally as “Bipolar III” — is what distinguishes cyclothymia from both bipolar II disorder (which requires at least one full hypomanic episode and one full major depressive episode) and major depressive disorder.
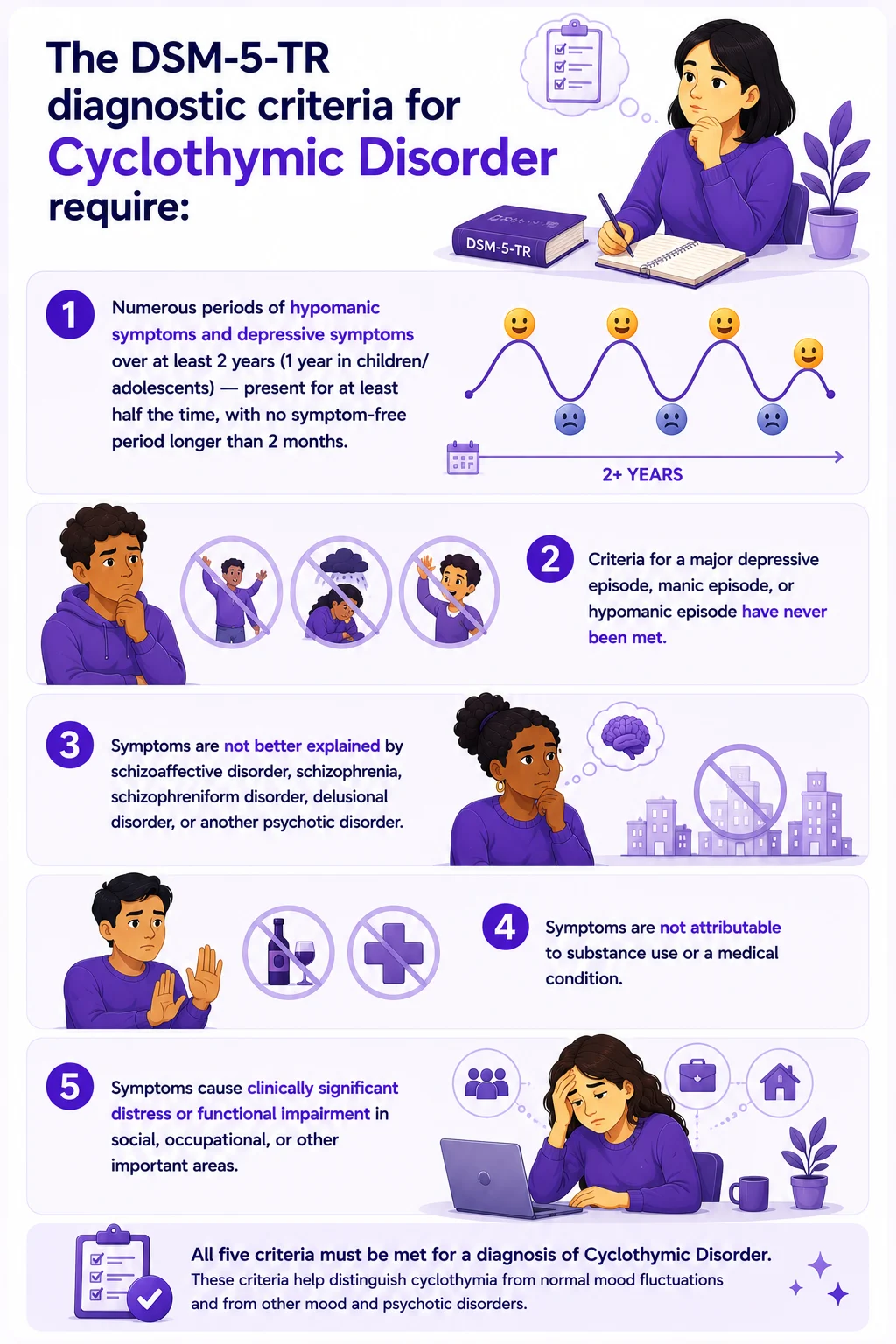
The DSM-5-TR diagnostic criteria for Cyclothymic Disorder require:
- Numerous periods of hypomanic symptoms and depressive symptoms over at least 2 years (1 year in children/adolescents) — present for at least half the time, with no symptom-free period longer than 2 months.
- Criteria for a major depressive episode, manic episode, or hypomanic episode have never been met.
- Symptoms are not better explained by schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder, or another psychotic disorder.
- Symptoms are not attributable to substance use or a medical condition.
- Symptoms cause clinically significant distress or functional impairment in social, occupational, or other important areas.
The prevalence of cyclothymia in the general population is estimated at 0.4–1%, though some research suggests that the cyclothymic temperament — a subclinical version of the same pattern — is far more common, affecting 5–6% of the population. Between 15–50% of individuals with cyclothymic disorder will go on to develop bipolar I or bipolar II disorder during their lifetime, making early identification clinically significant (APA, 2013; Theravive, 2024).
What Cyclothymia Actually Feels Like — Both Poles
Because cyclothymia operates below the clinical thresholds for full hypomanic or depressive episodes, it is frequently dismissed by clinicians, by the people around the person, and by the person themselves. The highs don’t look like mania. The lows don’t look like depression. From the outside, it can look like “just being moody.” From the inside, it looks like this:
The hypomanic-side periods. Not mania — but more than an ordinary good mood. There’s a distinct quality to it: a sense of expanded capacity, a reduced need for sleep without feeling tired, faster-moving thoughts that feel productive rather than scattered, and a pull toward projects, social contact, and new ideas. Confidence runs higher. Risk tolerance opens. You feel like the best version of yourself — sharper, more energetic, more interesting — and from the inside, this doesn’t feel like a symptom. It feels like clarity.
What makes it cyclothymia rather than ordinary productivity is that it is recurrent, noticeable as a departure from baseline, and followed by a shift downward. The person may look back on periods of high energy and recognize that they took on more than was sustainable, spent more than was wise, or made decisions that reflected the elevated state more than their considered judgment.
The depressive-side periods. Not major depression — but more than ordinary tiredness. A flatness. A withdrawal. Less energy, less interest, less motivation to engage with things that ordinarily feel rewarding. Social contact feels effortful. The future feels less available. Physical heaviness that sleep doesn’t fully resolve. Thoughts move more slowly, and the confidence of the high periods feels like a memory from someone else’s life.
Because these lows don’t reach the severity of major depression, they often go unrecognized as clinically significant — particularly because the person’s baseline experience has always included these shifts and the periods of elevation provide enough relief that the lows don’t accumulate into a recognizable depressive episode.
The cycling itself — what it costs. The pattern of continuous cycling is what produces the most significant functional impact. Relationships suffer because the person is perceptibly different across mood states — more engaged and confident in one, more withdrawn and flat in another. Commitments made in high periods exceed what low periods can sustain. The unpredictability makes it difficult to plan, maintain consistent work performance, and develop a stable sense of self. Many people with cyclothymia describe not knowing which “version” of themselves is the real one.
Cyclothymia vs. Bipolar II vs. Normal Mood Swings
The most clinically important distinctions for anyone questioning whether their mood cycling is cyclothymia are the comparisons with bipolar spectrum disorders on one end and ordinary mood variation on the other.
| Feature | Normal Mood Variation | Cyclothymia | Bipolar II Disorder | Bipolar I Disorder |
|---|---|---|---|---|
| High pole | Good mood — proportionate to circumstances | Hypomanic-level symptoms — does NOT meet full hypomanic criteria | Full hypomanic episode — meets DSM criteria, no hospitalization | Full manic episode — may require hospitalization |
| Low pole | Sadness — proportionate to circumstances, resolves | Depressive symptoms — does NOT meet full MDE criteria | A full major depressive episode is required for diagnosis | Major depressive episodes common but not required |
| Duration requirement | No minimum — resolves naturally | ≥2 years continuous cycling (≥1 year children) | No minimum duration for the disorder itself | No minimum duration for the disorder itself |
| Symptom-free periods | Extended symptom-free periods are normal | Never symptom-free for more than 2 months at a time | Symptom-free periods between episodes are possible | Symptom-free periods between episodes are possible |
| Severity | Mild, functional | Subthreshold but chronic — causes significant impairment | Moderate to severe — full episodes | Severe mania can be acutely dangerous |
| Progression risk | None | 15–50% risk of developing Bipolar I or II | May progress to Bipolar I | Most severe bipolar presentation |
| PsyMed screening | No screening needed | This test | Bipolar Test | Bipolar Test |
The progression risk deserves particular attention: between 15–50% of people with cyclothymia will eventually develop bipolar I or bipolar II disorder. This makes cyclothymia not just a condition worth treating in its own right, but a clinically significant risk marker for more severe bipolar spectrum presentations. Early identification and treatment meaningfully reduce the risk of progression.
What Causes Cyclothymia?
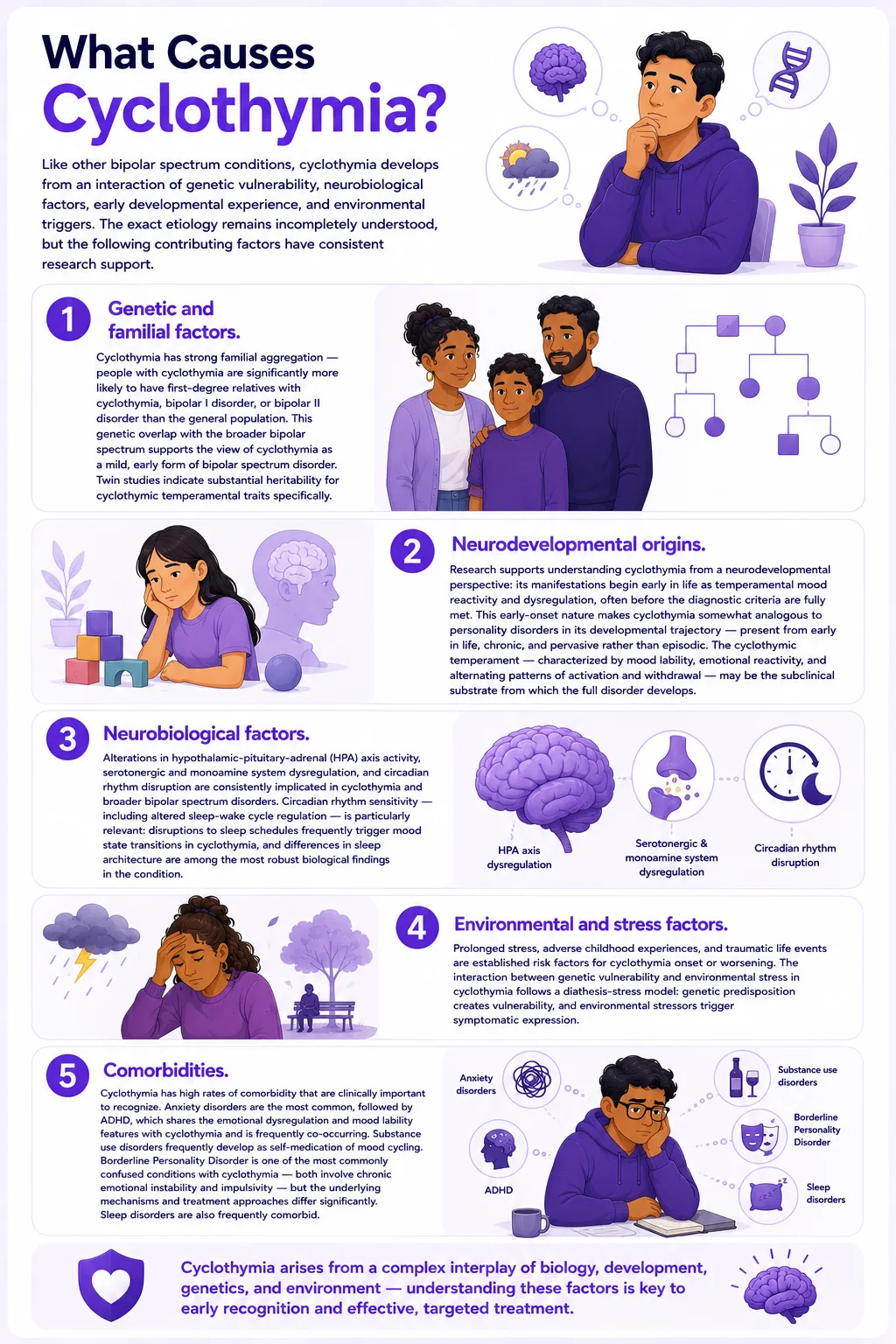
Like other bipolar spectrum conditions, cyclothymia develops from an interaction of genetic vulnerability, neurobiological factors, early developmental experience, and environmental triggers. The exact etiology remains incompletely understood, but the following contributing factors have consistent research support.
Genetic and familial factors. Cyclothymia has strong familial aggregation — people with cyclothymia are significantly more likely to have first-degree relatives with cyclothymia, bipolar I disorder, or bipolar II disorder than the general population. This genetic overlap with the broader bipolar spectrum supports the view of cyclothymia as a mild, early form of bipolar spectrum disorder. Twin studies indicate substantial heritability for cyclothymic temperamental traits specifically.
Neurodevelopmental origins. Research supports understanding cyclothymia from a neurodevelopmental perspective: its manifestations begin early in life as temperamental mood reactivity and dysregulation, often before the diagnostic criteria are fully met. This early-onset nature makes cyclothymia somewhat analogous to personality disorders in its developmental trajectory — present from early in life, chronic, and pervasive rather than episodic. The cyclothymic temperament — characterized by mood lability, emotional reactivity, and alternating patterns of activation and withdrawal — may be the subclinical substrate from which the full disorder develops.
Neurobiological factors. Alterations in hypothalamic-pituitary-adrenal (HPA) axis activity, serotonergic and monoamine system dysregulation, and circadian rhythm disruption are consistently implicated in cyclothymia and broader bipolar spectrum disorders. Circadian rhythm sensitivity — including altered sleep-wake cycle regulation — is particularly relevant: disruptions to sleep schedules frequently trigger mood state transitions in cyclothymia, and differences in sleep architecture are among the most robust biological findings in the condition.
Environmental and stress factors. Prolonged stress, adverse childhood experiences, and traumatic life events are established risk factors for cyclothymia onset or worsening. The interaction between genetic vulnerability and environmental stress in cyclothymia follows a diathesis-stress model: genetic predisposition creates vulnerability, and environmental stressors trigger symptomatic expression.
Comorbidities. Cyclothymia has high rates of comorbidity that are clinically important to recognize. Anxiety disorders are the most common, followed by ADHD, which shares the emotional dysregulation and mood lability features with cyclothymia and is frequently co-occurring. Substance use disorders frequently develop as self-medication of mood cycling. Borderline Personality Disorder is one of the most commonly confused conditions with cyclothymia — both involve chronic emotional instability and impulsivity — but the underlying mechanisms and treatment approaches differ significantly. Sleep disorders are also frequently comorbid.
How This Cyclothymia Test Works
This test screens for Cyclothymic Disorder using the DSM-5-TR diagnostic framework (APA, 2022) — covering both mood poles (hypomanic and depressive symptoms), the cycling pattern, and the functional impact and chronicity that distinguish cyclothymia from ordinary mood variation.
Answer based on your consistent experience over the past 2 years — not a single week or month, and not a specific episode, but the chronic recurring pattern across that period. The 2-year timeframe is clinically essential because it is the minimum duration criterion for the diagnosis of cyclothymia.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Total range: 0–60. This is a screening tool — it cannot diagnose Cyclothymic Disorder. A significant score is clinically meaningful and worth discussing with a qualified mental health professional, particularly a psychiatrist with experience in mood and bipolar spectrum disorders.
Understanding Your Cyclothymia Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Cyclothymia Indicators | Responses suggest few significant cyclothymic patterns. Normal mood variation may be present without a pattern consistent with Cyclothymic Disorder. |
| 16 – 30 | Mild — Some Mood Cycling Patterns Present | Some cyclothymic mood-cycling patterns are present on at least one pole. May not meet full cyclothymia criteria, but warrants monitoring and professional discussion. |
| 31 – 45 | Moderate — Significant Cyclothymic Pattern | Significant mood-cycling patterns are present at both poles. This pattern is consistent with Cyclothymic Disorder and warrants professional evaluation. |
| 46 – 60 | High — Strong Cyclothymia Indicators | Pervasive and chronic mood cycling across both poles with significant functional impact. Professional evaluation and support are strongly recommended. |
Treatment for Cyclothymia — What Works
Treatment for cyclothymia is less well-studied than for bipolar I and II disorder, primarily because the condition is less commonly identified and less severe per episode. However, evidence-based approaches exist and meaningfully improve outcomes — both in terms of quality of life with cyclothymia and in terms of reducing the risk of progression to a full bipolar disorder diagnosis.
Psychoeducation. Understanding the disorder is the foundation of effective treatment. Psychoeducation for cyclothymia covers: the nature of mood cycling and its neurobiological basis; identifying personal early warning signs for both mood poles; the relationship between sleep disruption, stress, and mood state transitions; lifestyle factors that stabilize or destabilize cycling; and realistic expectations about treatment. Research consistently shows that psychoeducation alone improves functional outcomes in bipolar spectrum disorders, including cyclothymia.
Interpersonal and Social Rhythm Therapy (IPSRT). Specifically developed for bipolar spectrum conditions, IPSRT combines interpersonal therapy with behavioral interventions targeting the social rhythms — regular sleep, meal times, activity schedules, and social contact patterns — that stabilize circadian rhythm function. Disruption to these rhythms is one of the most reliable triggers for mood cycling in cyclothymia, making rhythm stabilization a core treatment target.
Cognitive Behavioral Therapy (CBT). CBT adapted for bipolar spectrum conditions addresses the cognitive patterns that maintain and worsen mood cycling — including the maladaptive beliefs about high-energy periods (which may be overvalued as “real self”) and low periods (which may be catastrophized), and the behavioral patterns that reinforce cycling. CBT also targets the sleep disruption, impulsive decision-making, and interpersonal consequences that follow from unmanaged cycling.
Pharmacotherapy. No medications are specifically FDA-approved for cyclothymia. Evidence-supported options used in clinical practice include: lithium (best evidence across the bipolar spectrum, including cyclothymia); lamotrigine (particularly for the depressive pole); valproate/divalproex (mood stabilization); and quetiapine at low doses. Antidepressants are generally avoided as monotherapy in cyclothymia due to the risk of triggering or accelerating the hypomanic pole. Stimulant medications for comorbid ADHD require careful mood monitoring. A psychiatrist with bipolar spectrum experience should manage pharmacotherapy for cyclothymia.
Lifestyle and sleep management. Among the most clinically significant and accessible interventions for cyclothymia: maintaining regular sleep schedules (the most important single lifestyle factor for mood stability in bipolar spectrum disorders); limiting alcohol and recreational substance use; regular exercise; and structured daily routines that reduce the circadian irregularity that triggers cycling.
Frequently Asked Questions
What is cyclothymia?
Cyclothymia — formally Cyclothymic Disorder (DSM-5-TR 301.13 / F34.0) — is a chronic bipolar spectrum mood disorder characterized by recurrent periods of hypomanic-level symptoms and depressive-level symptoms over a minimum of two years, with no symptom-free interval exceeding two months. Unlike bipolar I or II disorder, neither mood pole reaches the full diagnostic threshold: hypomanic symptoms do not meet criteria for a full hypomanic episode, and depressive symptoms do not meet criteria for a major depressive episode. It affects approximately 0.4–1% of the general population and is sometimes informally referred to as “Bipolar III.” Between 15–50% of people with cyclothymia will develop bipolar I or II disorder during their lifetime.
What is the difference between cyclothymia and bipolar disorder?
The key distinction is severity and threshold. Bipolar I disorder requires at least one full manic episode. Bipolar II requires at least one full hypomanic episode and one full major depressive episode. Cyclothymia involves mood cycling that never reaches either of these full-episode thresholds — the highs are less severe than a full hypomanic episode, and the lows are less severe than a full major depressive episode. However, the cycling is chronic and continuous rather than episodic, which produces its own significant functional impact. Our Bipolar Test and Bipolar Depression Test cover the more severe spectrum presentations.
Can cyclothymia be mistaken for BPD?
Yes — and this is one of the most clinically significant diagnostic challenges in cyclothymia. Both cyclothymia and Borderline Personality Disorder (BPD) involve chronic emotional instability, mood cycling, impulsivity, and interpersonal difficulties. The key distinctions lie in the nature of the mood shifts: in BPD, mood shifts are typically triggered by interpersonal events and resolve within hours; in cyclothymia, mood states are more autonomous — they cycle regardless of external triggers and typically last days to weeks. Treatment approaches also differ significantly: BPD responds best to DBT and attachment-focused therapies; cyclothymia responds to mood stabilizers and IPSRT. Accurate diagnosis requires clinical evaluation — both conditions can co-occur.
Is cyclothymia a serious condition?
Yes — though it is less acutely severe than bipolar I or II disorder, cyclothymia is a chronic condition with significant functional impact. Research documents substantial impairment in occupational functioning, interpersonal relationships, and quality of life. The progression risk — 15–50% of people with cyclothymia will develop a full bipolar disorder — makes early identification and treatment clinically important. Cyclothymia is also associated with elevated rates of substance use disorders (often as self-medication), anxiety disorders, sleep disorders, and relationship difficulties. The chronic nature of the cycling means the cumulative burden over the years is significant even when individual episodes are mild.
What triggers cyclothymia mood swings?
The mood cycling in cyclothymia is partly autonomous — driven by the underlying neurobiological cycling pattern — and partly triggered by identifiable factors. The most reliably documented triggers include: sleep disruption and irregular sleep schedules (one of the strongest mood destabilizers in bipolar spectrum disorders); psychosocial stress; alcohol and substance use; seasonal changes; hormonal shifts; and major life transitions. Understanding personal triggers is a core component of cyclothymia treatment, as behavioral management of these triggers is among the most accessible and evidence-based interventions.
Can cyclothymia go away without treatment?
Cyclothymia follows a chronic course in most cases — it does not typically resolve spontaneously. Without treatment, the cycling tends to persist, functional impairment accumulates over time, and the risk of progression to a full bipolar disorder increases. With treatment — particularly psychoeducation, lifestyle modification, and appropriate pharmacotherapy — meaningful improvement in mood stability and functional outcomes is achievable. Many people with cyclothymia achieve substantial stabilization with treatment, though the condition typically requires ongoing management rather than a time-limited course of treatment.
Is cyclothymia related to ADHD?
There is a significant and clinically important relationship between cyclothymia and ADHD. Both conditions involve emotional dysregulation, mood lability, and difficulty with sustained attention and impulse control. Research shows they co-occur at higher-than-chance rates and share some neurobiological features related to dopaminergic regulation and executive function. The diagnostic distinction matters because treatment differs: stimulant medications for ADHD can destabilize mood cycling in cyclothymia if mood is not first stabilized. An integrated assessment covering both conditions is important for anyone with this symptom combination.
Related Tests
Cyclothymia overlaps clinically with several other conditions. These are the most relevant companion assessments:
- Bipolar Test — screens for full bipolar I and II presentations; important if mood episodes have ever reached full severity criteria
- Bipolar Depression Test — focuses specifically on the depressive pole of bipolar spectrum disorders; useful if the low periods are the more prominent feature
- Dysthymia Test — screens for Persistent Depressive Disorder; important to distinguish from the depressive pole of cyclothymia when low mood is chronic but cycling is minimal
- Clinical Depression Test — screens for major depressive disorder; important if depressive periods have ever reached full MDE severity
- Borderline Personality Disorder Test — one of the most commonly confused conditions with cyclothymia; both involve chronic emotional instability
- ADHD Test — frequently comorbid with cyclothymia; emotional dysregulation and mood lability overlap significantly between the two conditions
- Anxiety Test — anxiety disorders are the most common comorbidity of cyclothymia and affect treatment planning
- Burnout Test — burnout and the depressive pole of cyclothymia share significant symptom overlap; important to distinguish
- Edinburgh Postnatal Depression Scale (EPDS) — if you are pregnant or have recently given birth, cyclothymia significantly elevates perinatal mood risk; the EPDS is the validated screening tool for this period
For more mood disorder screenings, visit our Mood and Depression collection.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Cyclothymic Disorder 301.13 (F34.0). psychiatry.org
- Juruena, M.F., et al. (2017). Diagnosis and Treatment of Cyclothymia: The “Primacy” of Temperament. Current Neuropharmacology. PMC5405616. pmc.ncbi.nlm.nih.gov
- Samalin, L., et al. (2023). Cyclothymic Disorder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. NBK557877. ncbi.nlm.nih.gov
- Psychology Today. (2022). Cyclothymic Disorder. psychologytoday.com
- Theravive. (2024). Cyclothymic Disorder DSM-5 301.13 (F34.0). theravive.com
- ScienceDirect Topics. (2025). Cyclothymia. In: Encyclopedia of the Neurological Sciences, pp. 213–226. sciencedirect.com
- Baldessarini, R.J., Vázquez, G., & Tondo, L. (2011). Treatment of cyclothymic disorder: Commentary. Psychotherapy and Psychosomatics, 80(3), 131–135.
- Van Meter, A., & Youngstrom, E.A. (2012). Cyclothymia in youth: Why is it overlooked, what do we know and what is it? The Israel Journal of Psychiatry and Related Sciences, 49(1), 29–37.
- Lindner Center of Hope. (2025). Persistent Depressive Disorder and Cyclothymic Disorder. lindnercenterofhope.org