
If you’re in crisis or thinking about suicide, please reach out now.
📞 988 Suicide & Crisis Lifeline — Call or text 988 (US, 24/7)
💬 Crisis Text Line — Text TALK to 741741
Bipolar disorder carries elevated suicide risk, especially during depressive and mixed episodes. If you’re in immediate danger, go to your nearest emergency room.
The highs can feel like a gift at first. You need less sleep and feel sharper for it. Your ideas connect faster than usual. You feel capable of things your ordinary self wouldn’t attempt. The productivity, the confidence, the sense that everything is finally clicking — these feel like your best self, not a symptom. The lows that follow feel like the only real version of you.
This reversal — believing the depression is who you actually are, while the highs were something else — is one of the reasons bipolar disorder goes undiagnosed for an average of five to ten years after symptom onset. Most people seek help during the low periods, describe only the depression, and receive treatment for unipolar depression that doesn’t address — and may actually worsen — the underlying bipolar condition.
This free Bipolar Test screens for Bipolar I, Bipolar II, and Cyclothymia using DSM-5-TR criteria (APA, 2022). 20 questions covering both mood poles. Instant, private results.
What Is Bipolar Disorder?
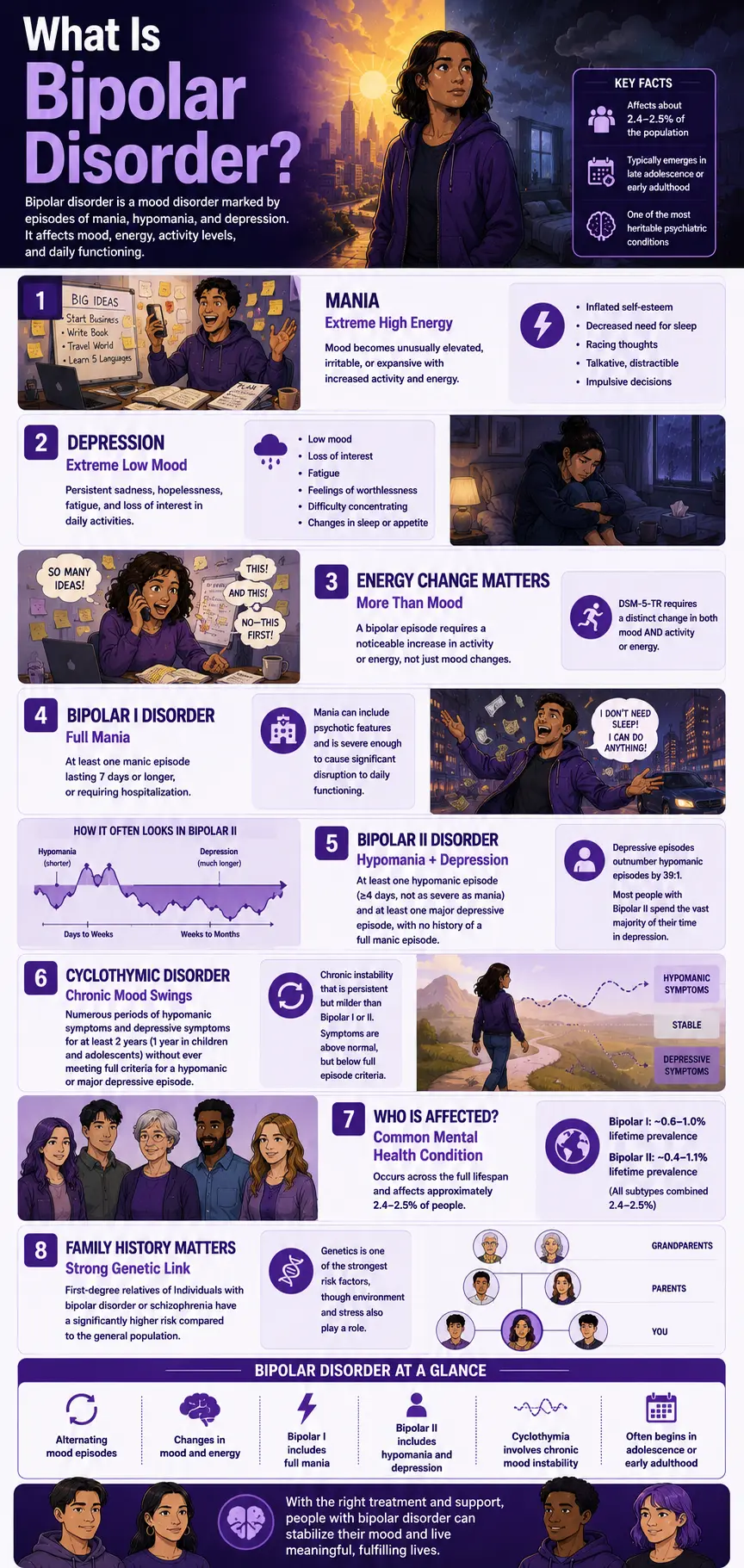
Bipolar disorder — formerly known as manic-depressive illness — is a mood disorder characterized by distinct episodes of mania or hypomania (elevated, expansive, or irritable mood with increased energy) alternating with episodes of major depression. It is one of the most heritable psychiatric conditions, with first-degree relatives of individuals with bipolar disorder or schizophrenia having significantly higher prevalence rates than the general population (HealthCentral, 2020, citing DSM-5 data).
Bipolar disorder occurs across the full lifespan but typically emerges in late adolescence or early adulthood. It affects approximately 2.4–2.5% of the population across all subtypes combined (World Mental Health Survey Initiative, Merikangas et al., Archives of General Psychiatry, 2011), with Bipolar I at ~0.6–1.0% and Bipolar II at ~0.4–1.1% lifetime prevalence (World Mental Health Survey, PMC; clinical trials data).
A critical DSM-5-TR revision clarified that a manic or hypomanic episode requires not only a distinct change in mood but also a distinct change in activity or energy — the activity/energy increase is now a required criterion alongside the mood change, not just a supporting symptom (APA, DSM-5 Changes, 2013). This change was significant: it means that mood elevation alone is not sufficient for a manic or hypomanic diagnosis.
The three primary diagnoses on the bipolar spectrum:
Bipolar I Disorder (DSM-5-TR 296.xx) is defined by at least one full manic episode lasting 7 days or more — or less if hospitalization is required. Depressive episodes are common but are not required for diagnosis. Bipolar I mania can include psychotic features and is severe enough to cause significant disruption to daily functioning.
Bipolar II Disorder (DSM-5-TR 296.89) is defined by at least one hypomanic episode (a less intense form, lasting ≥4 days, without hospitalization or psychotic features) and at least one major depressive episode, with no history of a full manic episode. Bipolar II is frequently missed because hypomania can feel productive and positive. Importantly, depressive episodes in Bipolar II outnumber hypomanic episodes by a ratio of 39:1 (Berk et al., World Psychiatry, 2025) — meaning most people with Bipolar II spend the vast majority of their symptomatic time in depression, not hypomania.
Cyclothymic Disorder (DSM-5-TR 301.13) is a chronic, milder form characterized by numerous periods of hypomanic symptoms and depressive symptoms over at least 2 years (1 year in children and adolescents) without ever meeting full criteria for a hypomanic or major depressive episode. The instability is constant but below the severity thresholds of Bipolar I or II.
Signs You Might Have Bipolar Disorder
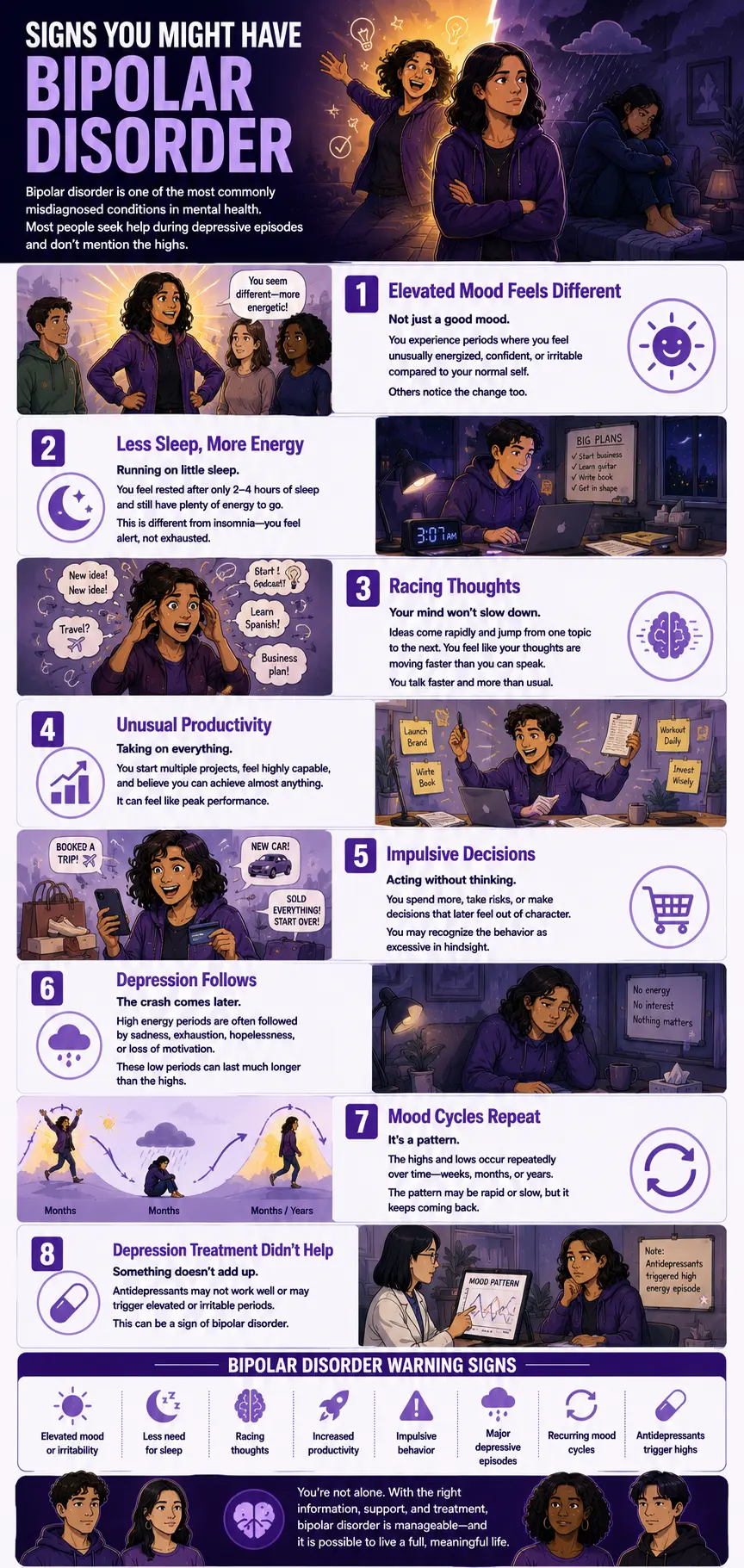
Bipolar disorder is one of the most commonly misdiagnosed conditions in mental health — partly because most people seek help during depressive episodes and don’t mention the highs, and partly because the manic and hypomanic periods often don’t feel like symptoms. These are the patterns that most consistently indicate bipolar disorder may be present:
You have experienced distinct periods of elevated or irritable mood that felt qualitatively different from your normal self — not just “a good mood” but a different operating state. The manic or hypomanic state is not simply happiness or confidence. It is a distinct episode — a noticeable departure from your baseline that others observe as well as you experience. The key DSM-5-TR requirement is that this represents a change from the person’s usual behavior, not just a temporary positive mood.
During these elevated periods, you needed significantly less sleep without feeling tired. Decreased need for sleep — not insomnia, but genuinely feeling rested and energized after only 2–4 hours — is one of the most specific and reliable markers of a manic or hypomanic episode. This is not the same as being unable to sleep due to anxiety. It is feeling fully rested and alert despite dramatically shortened sleep.
Your thoughts raced, your ideas multiplied rapidly, and you felt like your mind was outpacing your ability to express it. Flight of ideas — the rapid sequence of thoughts jumping from one topic to the next with loose associations — and pressured speech (talking faster, more, and more intensely than usual) are characteristic manic features. The person often describes feeling like they can’t get their thoughts out fast enough.
You were unusually productive, took on multiple projects, or felt capable of achievements that exceeded your normal confidence. The increase in goal-directed activity and inflated self-esteem that characterize mania can look like peak performance in the early stages. The grandiosity may feel like realistic confidence rather than distortion.
You made impulsive decisions during these high periods that you later recognized as out of character. Spending sprees, sexual indiscretions, risky investments, substance use, or other impulsive behavior that the person would not consider during their baseline state. The behavior is driven by the elevated mood state and is typically recognized as excessive in retrospect.
These elevated periods are followed by — or alternate with — periods of significant depression. Both Bipolar I and Bipolar II patients spend approximately three times more days in depression than in mania or hypomania (Kupka et al., 2007, cited in Berk et al., World Psychiatry, 2025). The depression in bipolar disorder is often indistinguishable on the surface from unipolar depression — it is the history of elevated episodes that differentiates it.
The pattern has been cyclical and persistent — not a single episode but a recurring pattern. Bipolar disorder produces episodes over time. A single manic episode may be followed by years of relative stability or by regular cycling. The characteristic pattern — whether rapid or slow, whether primarily depressive or primarily manic — is what creates the clinical picture over time.
You have been treated for depression but the treatment hasn’t worked well, or may have triggered elevated periods. Antidepressants used in bipolar disorder without mood stabilizers can trigger manic or hypomanic episodes or worsen the cycling pattern. A history of antidepressants triggering elevation is itself a DSM-5-TR-recognized indicator of possible bipolar disorder.
Bipolar I vs Bipolar II vs Cyclothymia vs Unipolar Depression
| Feature | Bipolar I | Bipolar II | Cyclothymia | Unipolar Depression (MDD) |
|---|---|---|---|---|
| Elevated mood episodes | Full mania: ≥7 days, severe, may require hospitalization or involve psychosis | Hypomania only: ≥4 days, less severe, no hospitalization, no psychosis | Hypomanic symptoms: present but never meeting full hypomanic episode criteria | None — diagnosis requires no history of mania or hypomania |
| Depressive episodes | Common but not required for diagnosis; may be severe | Required for diagnosis; typically the predominant feature (39:1 ratio over hypomania) | Depressive symptoms are present but never meet full MDE criteria | Required — defines the disorder; no upper pole |
| DSM-5-TR code | 296.xx | 296.89 | 301.13 | 296.xx |
| Antidepressant risk | HIGH — can trigger severe mania without a mood stabilizer | MODERATE-HIGH — can trigger hypomania or cycling | MODERATE — monitoring recommended | Standard use — not associated with manic switching |
| Most misdiagnosed as | Schizophrenia (when psychotic features are present) or MDD | Unipolar depression — most commonly missed as bipolar type | Borderline PD, ADHD, or unipolar depression | Sometimes misidentified as Bipolar II if depressive episodes are severe |
| Mood stabilizers | Essential — lithium, valproate, antipsychotics | Essential — especially if antidepressants are used | Recommended for ongoing stability | Not typically required |
| PsyMed test | This test | This test | Cyclothymia Test | Clinical Depression Test |
Important: Bipolar disorder is associated with a significantly elevated risk of suicide. If you’re having thoughts of suicide or self-harm, please reach out now — call or text 988 (US, 24/7). You don’t have to be in crisis to call.
What Causes Bipolar Disorder?
Bipolar disorder is among the most heritable psychiatric conditions. Its etiology is primarily biological, with environmental factors shaping onset and course.
Genetic factors. Bipolar disorder has among the highest heritability of any psychiatric condition — estimated at 60–80% in twin studies. First-degree relatives of individuals with Bipolar I or Bipolar II have significantly elevated rates compared to the general population (HealthCentral, 2020, citing DSM-5 data). Shared genetic architecture with schizophrenia has been documented in genome-wide association studies.
Neurobiological factors. Dysregulation in monoamine neurotransmitter systems — particularly dopamine, serotonin, and norepinephrine — is well-documented in bipolar disorder. Lithium and other mood stabilizers are believed to work through multiple pathways, including neuroprotection, modulation of the glutamate system, and second-messenger signaling. Neuroimaging studies show structural and functional differences in the prefrontal cortex, amygdala, and other mood-regulating regions.
Circadian rhythm disruption. Disruption of the sleep-wake cycle is both a symptom and a precipitant of bipolar episodes. The decreased need for sleep in mania and hypersomnia in depression reflect circadian dysregulation that is intrinsic to the disorder. Social Rhythm Therapy — a component of Interpersonal and Social Rhythm Therapy (IPSRT) — specifically addresses this by stabilizing daily routines.
Environmental triggers. Life events — particularly sleep disruption, major stressors, and goal attainment events — can trigger episodes in genetically vulnerable individuals. Substance use (particularly stimulants and cannabis) can precipitate manic episodes or worsen cycling.
Comorbidities. Bipolar disorder has very high comorbidity rates. Anxiety disorders are among the most common comorbidities. ADHD is frequently comorbid — and frequently confused with bipolar disorder given shared features of impulsivity and mood instability. Borderline Personality Disorder shares emotional dysregulation and impulsivity with bipolar disorder and is a common differential. Substance use disorders and major depressive disorder comorbidities significantly complicate treatment.
How This Test Works
This Bipolar Test covers both mood poles — manic/hypomanic symptoms (Questions 1–10) and depressive symptoms (Questions 11–20) — across 20 questions. It is based on the DSM-5-TR diagnostic criteria for manic episodes, hypomanic episodes, and major depressive episodes (APA, 2022).
Important note on interpretation: Because this test covers both poles, a high score driven primarily by depressive symptoms alone — without elevated mood, decreased sleep, racing thoughts, or impulsive behavior — may indicate unipolar depression rather than bipolar disorder. The results below address this nuance. Only a clinical professional can determine the correct diagnosis.
Answer based on your experience of distinct episodes over your lifetime — not your current mood, but recurring patterns you have experienced. For manic/hypomanic questions, consider whether these experiences occurred during discrete periods that were different from your normal baseline.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–80. This is a screening tool only.
Understanding Your Bipolar Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 20 | Low — Few Bipolar Indicators | Responses suggest few significant bipolar disorder patterns. Mood variation present without a pattern consistent with bipolar disorder criteria. |
| 21 – 40 | Mild — Some Mood Episode Patterns | Some mood episode patterns are present. May reflect subthreshold bipolar features, Cyclothymia, or other mood conditions. Worth professional discussion. |
| 41 – 60 | Moderate — Significant Mood Episode Pattern | Significant mood episode patterns across multiple criteria. Consistent with the possible bipolar disorder spectrum, professional evaluation is recommended. |
| 61 – 80 | High — Strong Bipolar Indicators | Pervasive and severe mood episode patterns across most criteria. Professional evaluation is strongly recommended as soon as possible. |
Treatment for Bipolar Disorder
Bipolar disorder is highly treatable. The majority of people with bipolar disorder achieve good symptom control and maintain functional lives with appropriate treatment.
Mood stabilizers — first-line pharmacotherapy. Lithium is the most evidence-supported mood stabilizer for Bipolar I and has the strongest evidence for reduction of suicide risk in bipolar disorder. Valproate (valproic acid) and carbamazepine are effective alternatives, particularly for rapid cycling or mixed states. Lamotrigine has particular evidence for the prevention of bipolar depressive episodes.
Atypical antipsychotics. Several atypical antipsychotics (quetiapine, olanzapine, aripiprazole) are FDA-approved for bipolar disorder and are used for both acute episodes and maintenance treatment.
Cognitive Behavioral Therapy for Bipolar Disorder (CBT-BD). Specifically adapted for bipolar disorder, CBT-BD targets the maladaptive thought patterns and behaviors that contribute to episode maintenance and builds skills for identifying early warning signs of impending episodes.
Interpersonal and Social Rhythm Therapy (IPSRT). Developed specifically for bipolar disorder, IPSRT addresses the circadian rhythm disruption that both precipitates and maintains bipolar episodes — by stabilizing daily routines, sleep schedules, and social rhythms. Strong evidence base as an adjunctive treatment.
Psychoeducation. Evidence consistently shows that comprehensive psychoeducation about bipolar disorder — including understanding episode triggers, early warning signs, and the rationale for medication adherence — significantly improves long-term outcomes.
Frequently Asked Questions
What is bipolar disorder?
Bipolar disorder is a mood disorder characterized by distinct episodes of mania or hypomania (elevated, expansive, or irritable mood with increased energy/activity) alternating with episodes of major depression. The three primary DSM-5-TR diagnoses are Bipolar I (296.xx) — defined by at least one full manic episode; Bipolar II (296.89) — defined by at least one hypomanic episode plus at least one major depressive episode with no history of mania; and Cyclothymic Disorder (301.13) — a chronic, milder form with hypomanic and depressive symptoms below full episode thresholds for ≥2 years. Across all subtypes, the bipolar spectrum affects approximately 2.4–2.5% of the population (World Mental Health Survey).
What is the difference between mania and hypomania?
Mania and hypomania share the same symptom profile — elevated/expansive/irritable mood plus increased energy/activity, with ≥3 of 7 DIGFAST criteria (≥4 with irritable mood) — but differ in severity, duration, and consequences. Mania lasts ≥7 days (or requires hospitalization), may include psychotic features, and is severe enough to cause significant functional impairment. Hypomania lasts ≥4 days, does not require hospitalization, and does not include psychotic features. Critically, the DSM-5-TR specifies that hypomania is “not severe enough to cause marked impairment in social or occupational functioning or to necessitate hospitalization” — if those thresholds are crossed, the episode is classified as manic, not hypomanic, regardless of the person’s subjective experience of it.
Why is bipolar disorder so commonly misdiagnosed?
Bipolar disorder is misdiagnosed primarily because most people seek help during depressive episodes, describe only the depression, and do not volunteer — or do not recognize — their history of elevated episodes. Clinicians who don’t specifically ask about hypomanic periods will not discover them. Bipolar II is particularly vulnerable to misdiagnosis as unipolar depression because the hypomanic episodes may be experienced as positive — productive, energetic, social — rather than as a symptom requiring treatment. The average delay from symptom onset to correct diagnosis is five to ten years. In Bipolar II specifically, depressive episodes outnumber hypomanic episodes by 39:1 (Berk et al., World Psychiatry, 2025), meaning most of the clinical presentation is depression.
Can antidepressants be used for bipolar depression?
This is one of the most clinically important questions in bipolar treatment. Antidepressants used alone — without a concurrent mood stabilizer — in bipolar disorder carry a risk of triggering manic or hypomanic episodes, accelerating cycling, or producing a mixed state. The DSM-5-TR recognizes that antidepressant-induced elevation that persists beyond the drug’s physiological effect is evidence of Bipolar II. Current treatment guidelines generally recommend against antidepressant monotherapy for bipolar depression and favor mood stabilizers (particularly lamotrigine for bipolar depression) with or without adjunctive antidepressants and with close monitoring. This is one of the key reasons correct diagnosis is so important — being treated for unipolar depression when the actual condition is bipolar can worsen the underlying condition.
What is the difference between bipolar disorder and borderline personality disorder?
BPD and bipolar disorder share emotional dysregulation, impulsivity, and mood instability — and are among the most commonly confused diagnoses. The key distinctions: bipolar disorder involves distinct episodes (states that last days to weeks and represent a change from baseline), while BPD involves pervasive emotional instability that is more reactive to interpersonal triggers and doesn’t follow an episodic pattern. The mood shifts in BPD tend to occur within hours in response to perceived rejection or interpersonal conflict; the mood shifts in bipolar disorder occur over days to weeks and may have no clear precipitant. Both conditions can co-occur. The Borderline Personality Disorder Test is worth completing alongside this one.
Can you have bipolar disorder and ADHD at the same time?
Yes — ADHD and bipolar disorder co-occur significantly more often than expected by chance, and the two conditions share several surface features: impulsivity, distractibility, mood variability, and periods of increased activity. The key distinctions: ADHD features are chronic and pervasive (present across all contexts and throughout development), while bipolar features are episodic (distinct from the person’s baseline). ADHD impulsivity is not driven by elevated mood or decreased sleep need. Correct differentiation matters for treatment: stimulant medications used for ADHD can trigger manic episodes in bipolar disorder, so bipolar disorder should be ruled out or treated first. Complete the ADHD Test alongside this one if impulsivity and distractibility are prominent features.
What is Cyclothymia?
Cyclothymic Disorder (DSM-5-TR 301.13) is a chronic mood condition characterized by numerous periods of hypomanic symptoms and depressive symptoms over at least 2 years (1 year for children and adolescents), without ever meeting the full criteria for a hypomanic episode or a major depressive episode. The mood instability is constant but below the severity thresholds of Bipolar I or II. Cyclothymia is often undiagnosed because neither the highs nor the lows are severe enough to feel like a “real” disorder — but the chronic instability is exhausting and significantly affects quality of life. Cyclothymia may be a precursor to Bipolar I or II in some individuals. The dedicated Cyclothymia Test screens specifically for this presentation.
Related Tests
- Cyclothymia Test — screens specifically for the chronic, subthreshold mood cycling of Cyclothymic Disorder; most relevant if mood instability is present but below full bipolar episode thresholds
- Clinical Depression Test — essential companion; bipolar depression and unipolar depression present identically on the surface; ruling out bipolar disorder before treating for unipolar depression is clinically critical
- Dysthymia Test — persistent depressive disorder; chronic low-grade depression that can occur alongside or be confused with cyclothymia
- Borderline Personality Disorder Test — most commonly confused with bipolar disorder; shares emotional dysregulation and impulsivity through different mechanisms
- ADHD Test — frequently comorbid with and confused with bipolar disorder; shares impulsivity and mood variability features
- Anxiety Test — anxiety disorders are among the most common bipolar comorbidities
- Anhedonia Test — loss of pleasure is a core bipolar depressive feature worth assessing separately
- High Functioning Depression Test — some people with Bipolar II maintain external function despite severe depressive episodes; worth exploring
- Suicidal Ideation Test — bipolar disorder, particularly Bipolar II and mixed states, carries elevated suicide risk; please assess if suicidal thoughts have been present during depressive episodes
- Imposter Syndrome Test — some people attribute their hypomanic confidence to imposter syndrome in retrospect; worth distinguishing
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Bipolar and Related Disorders. psychiatry.org
- Berk, M., Corrales, A., Trisno, R., et al. (2025). Bipolar II disorder: a state-of-the-art review. World Psychiatry, 24(2), 175–189. [39:1 depressive: hypomanic episode ratio] doi.org/10.1002/wps.21300
- Merikangas, K.R., Jin, R., He, J.P., et al. (2011). Prevalence and correlates of bipolar spectrum disorder in the World Mental Health Survey Initiative. Archives of General Psychiatry, 68(3), 241–251. [2.4% spectrum prevalence] pmc.ncbi.nlm.nih.gov
- Kupka, R.W., Altshuler, L.L., Nolen, W.A., et al. (2007). Three times more days are depressed than manic or hypomanic in both bipolar I and bipolar II disorders. Bipolar Disorders, 9(5), 531–535. [3x more days depressed] Cited in Berk et al. 2025.
- American Psychiatric Association. (2013). Highlights of Changes from DSM-IV-TR to DSM-5. [Activity/energy added as required criterion; agoraphobia-panic separation] psychiatry.org
- Statpearls. Bipolar Disorder. NCBI Bookshelf. NBK558998. ncbi.nlm.nih.gov
- HealthCentral. (2020). Bipolar Definition and DSM-5 Diagnostic Criteria. [2.5% population; first-degree relative risk] healthcentral.com
- Wikipedia. (2025). Bipolar disorder. en.wikipedia.org