
“ADD” — Attention Deficit Disorder — is the term millions of people still use for the kind of attention difficulty that doesn’t come with obvious hyperactivity: the quiet daydreamer, the person who reads the same paragraph five times, the one who walks into a room and forgets why. Here’s something important to know up front: “ADD” is no longer an official medical diagnosis. What was once called ADD is now understood as a form of ADHD — specifically, ADHD, predominantly inattentive presentation. The name changed, but the experience it describes is very real.
If you struggle to sustain focus, lose track of tasks, drift off mid-conversation, forget appointments, or find it hard to finish what you start — even when you genuinely want to — this free ADD Test (Attention Deficit Disorder Test) can help you understand your attention patterns. It screens for both inattentive traits (the core of what people call “ADD”) and hyperactive-impulsive traits, using criteria adapted from the DSM-5-TR (APA, 2022). 15 questions, for teens and adults. Instant, private results.
This test is a screening tool, not a diagnosis. If your results suggest significant attention difficulties, a qualified healthcare professional can provide a proper evaluation. If you’d like a more comprehensive screen across all three ADHD presentations, take our Free ADHD Test, designed specifically for adults.
What Is Attention Deficit Disorder (ADD)?
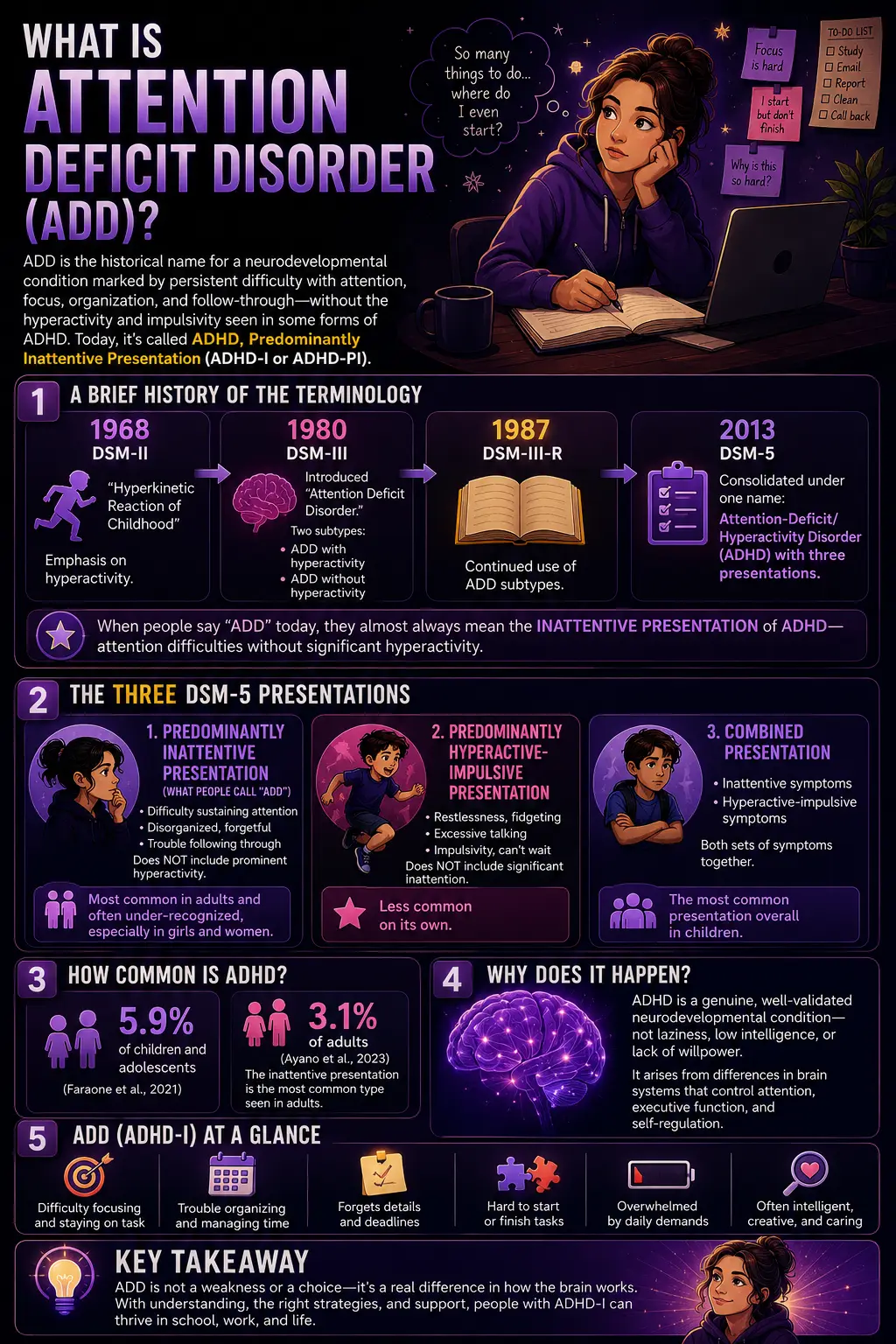
Attention Deficit Disorder (ADD) is the historical and still-common name for a neurodevelopmental condition characterized by persistent difficulty with attention, focus, organization, and follow-through — without the prominent hyperactivity and impulsivity that many people associate with ADHD. In current clinical terminology, this is called ADHD, predominantly inattentive presentation (sometimes abbreviated ADHD-I or ADHD-PI).
The terminology has a history worth understanding, because it explains why “ADD” and “ADHD” are both still used. The condition was first formally described as “Hyperkinetic Reaction of Childhood” in the DSM-II (1968), with the emphasis on hyperactivity. In 1980, the DSM-III shifted the focus to attention and introduced the term “Attention Deficit Disorder,” with two subtypes: ADD with hyperactivity and ADD without hyperactivity. In 1987 (DSM-III-R) and definitively in the DSM-5 (2013), the diagnosis was consolidated under a single name — Attention-Deficit/Hyperactivity Disorder (ADHD) — with three “presentations” rather than separate disorders (Frontiers in Psychology, 2025).
So when someone says they have “ADD” today, they almost always mean what clinicians now call the inattentive presentation of ADHD — attention difficulties without significant hyperactivity. This is one of the three DSM-5 presentations:
Predominantly inattentive presentation (what people call “ADD”) — difficulty sustaining attention, organizing, following through, and remembering, without prominent hyperactivity. It is the most common presentation in adults and is frequently under-recognized, especially in girls and women, because it doesn’t produce disruptive behavior.
Predominantly hyperactive-impulsive presentation — restlessness, fidgeting, excessive talking, impulsivity, and difficulty waiting, without significant inattention. Less common on its own.
Combined presentation — both inattentive and hyperactive-impulsive symptoms together. The most common presentation overall in children.
ADHD affects approximately 5.9% of children and adolescents (Faraone et al., 2021) and around 3.1% of adults, with the inattentive presentation being the most common type seen in adults (Ayano et al., 2023). It is a genuine, well-validated neurodevelopmental condition — not a matter of laziness, low intelligence, or insufficient willpower. The difficulties arise from differences in brain systems governing attention, executive function, and self-regulation.
ADD vs ADHD — What’s the Difference?
This is the most common question people have, and the answer is simpler than the terminology suggests: ADD is an older name for what is now called the inattentive presentation of ADHD. They are not two different conditions — ADD is, in effect, ADHD without the hyperactivity.
| Feature | “ADD” (Inattentive Presentation) | ADHD (Hyperactive-Impulsive or Combined) |
|---|---|---|
| Current clinical term | ADHD, predominantly inattentive presentation | ADHD, hyperactive-impulsive or combined presentation |
| Core difficulties | Focus, organization, memory, follow-through, distractibility | Restlessness, fidgeting, impulsivity, excessive talking (plus inattention in combined) |
| Visibility | Often quiet and internal; easily missed, especially in girls/women and adults | More outwardly visible and disruptive; more often noticed early |
| Typical presentation | Daydreaming, “spacey,” forgetful, disorganized, slow to start tasks | “On the go,” can’t sit still, interrupts, acts before thinking |
| Is it a separate condition? | No — it’s one of three presentations of ADHD in the DSM-5 | No — same diagnosis, different presentation |
| PsyMed test | This ADD Test (inattentive focus) | ADHD Test (all presentations) |
Why does the old term “ADD” persist? Partly habit, and partly because for people with the inattentive presentation, “Attention Deficit Hyperactivity Disorder” feels inaccurate — they don’t experience hyperactivity. Many people find “ADD” a more fitting description of their quiet, internal experience of attention difficulty. Both terms point to the same underlying condition; “ADD” simply emphasizes the inattentive side.

Signs You Might Have ADD (Inattentive ADHD)
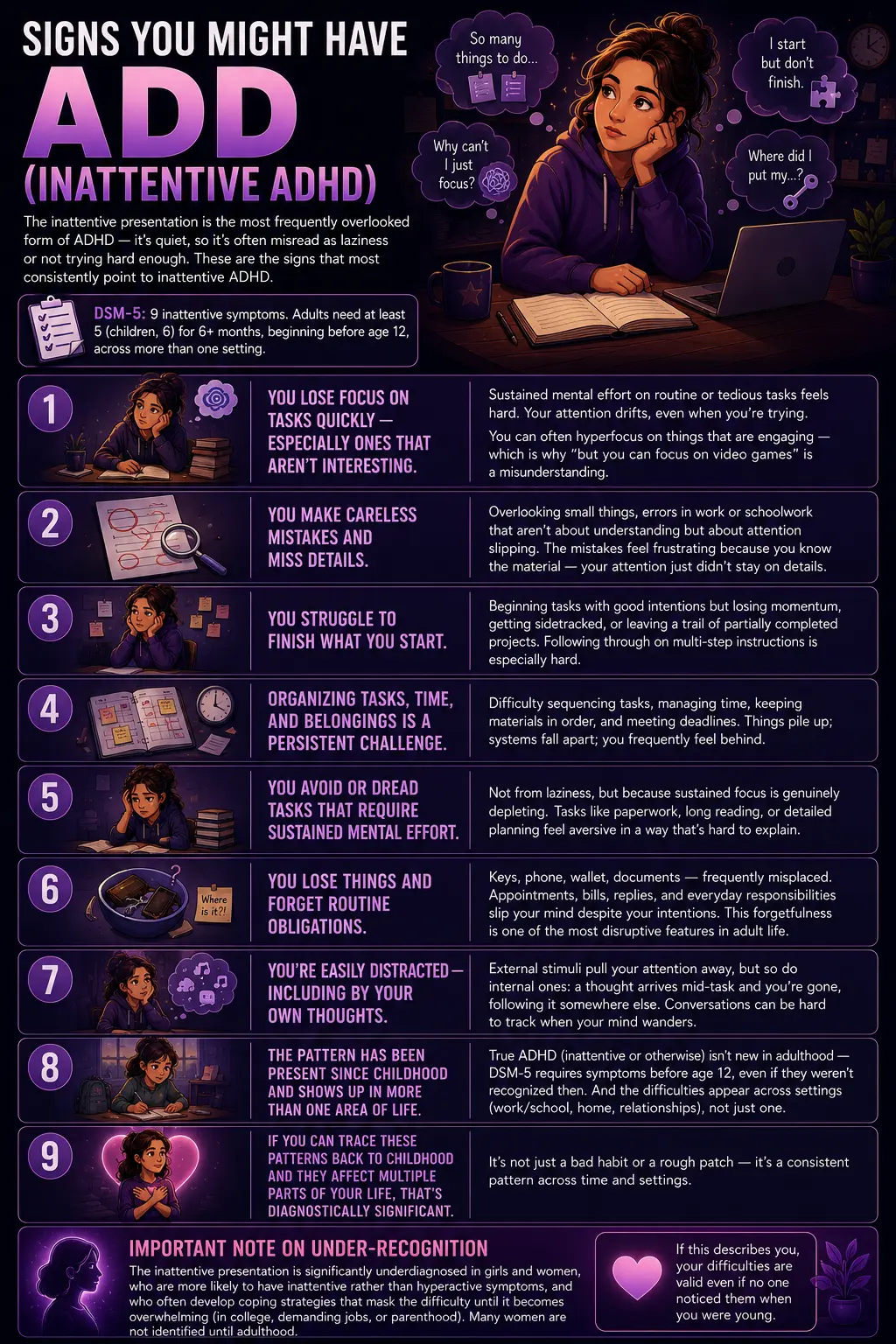
The inattentive presentation is the most frequently overlooked form of ADHD, precisely because it’s quiet. There’s no disruptive behavior to draw attention — just a persistent, private struggle that’s often misread as laziness, carelessness, or not trying hard enough. These are the signs that most consistently point to inattentive ADHD. The DSM-5 lists nine inattentive symptoms; adults need at least five (children, six) present for six or more months, beginning before age 12, across more than one setting.
You lose focus on tasks quickly — especially ones that aren’t inherently interesting. Sustained mental effort on routine or tedious tasks feels disproportionately hard. Your attention drifts, even when you’re trying to concentrate and the task matters. (Notably, people with ADHD can often hyperfocus on things that are engaging — which is why “but you can focus on video games” is a misunderstanding of how ADHD attention works.)
You make careless mistakes and miss details. Overlooking small things, errors in work or schoolwork that aren’t about understanding but about attention slipping. The mistakes feel frustrating because you know the material — your attention just didn’t stay on the details.
You struggle to finish what you start. Beginning tasks with good intentions but losing momentum, getting sidetracked, or leaving a trail of partially completed projects. Following through on multi-step instructions is especially hard.
Organizing tasks, time, and belongings is a persistent challenge. Difficulty sequencing tasks, managing time, keeping materials in order, and meeting deadlines. Things pile up; systems fall apart; you frequently feel behind.
You avoid or dread tasks that require sustained mental effort. Not from laziness, but because sustained focus is genuinely depleting. Tasks like paperwork, long reading, or detailed planning feel aversive in a way that’s hard to explain to others.
You lose things and forget routine obligations. Keys, phone, wallet, documents — frequently misplaced. Appointments, bills, replies, and everyday responsibilities slip your mind despite your intentions. This forgetfulness is one of the most disruptive features in adult life.
You’re easily distracted — including by your own thoughts. External stimuli pull your attention away, but so do internal ones: a thought arrives mid-task and you’re gone, following it somewhere else. Conversations can be hard to track when your mind wanders.
The pattern has been present since childhood and shows up in more than one area of life. True ADHD (inattentive or otherwise) isn’t new in adulthood — the DSM-5 requires that several symptoms were present before age 12, even if they weren’t recognized at the time. And the difficulties appear across settings (work/school, home, relationships), not just one. If you can trace these patterns back to childhood and they affect multiple parts of your life, that’s diagnostically significant.
An important note on under-recognition: the inattentive presentation is significantly underdiagnosed in girls and women, who are more likely to have inattentive rather than hyperactive symptoms, and who often develop coping strategies that mask the difficulty until it becomes overwhelming (in college, in demanding jobs, or in parenthood). Many women are not identified until adulthood. If this describes you, your difficulties are valid even if no one noticed them when you were young.
How This ADD Test Works
This ADD Test contains 15 questions covering both symptom domains the DSM-5 uses for ADHD: nine questions on inattention (the core of what people call “ADD”) and six on hyperactivity-impulsivity. This structure lets the test reflect not just whether attention difficulties are present, but whether your pattern leans toward the purely inattentive (“ADD”) presentation or includes hyperactive-impulsive traits as well.
For each question, choose how often the experience applies to you, based on your behavior and feelings over recent months: Never, Rarely, Sometimes, Often, or Constantly.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Constantly = 4
Total range: 0–60. Answer honestly — and keep in mind that a genuine ADHD pattern involves symptoms that have been present since childhood (before age 12), occur in more than one setting, and cause real difficulty in daily life. This is a screening tool, not a diagnosis.
Understanding Your ADD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Minimal — Few Attention Indicators | Few signs of clinically significant attention difficulty. Everyday lapses in focus may be present within the normal range. |
| 16 – 30 | Mild — Some Attention Difficulties | Some attention or hyperactivity-impulsivity traits are present. Worth monitoring and discussing with a professional if they affect daily life. |
| 31 – 45 | Moderate — Significant Attention Difficulties | Meaningful attention difficulties consistent with ADHD. Professional evaluation is recommended to clarify and address them. |
| 46 – 60 | High — Strong ADHD Indicators | Strong indicators consistent with ADHD across multiple symptoms. A professional evaluation is strongly recommended. |
What Causes ADHD?
ADHD is one of the most heritable psychiatric conditions, with genetics accounting for a substantial proportion of risk — heritability estimates are around 74%. It tends to run in families, and having a first-degree relative with ADHD significantly increases the likelihood. Neurobiologically, ADHD involves differences in brain structure, function, and connectivity — particularly in the frontostriatal and frontoparietal networks that govern attention, executive function, and impulse control — and in the dopamine and norepinephrine neurotransmitter systems, which is why medications targeting these systems are effective.
Environmental and prenatal factors can contribute to risk, including premature birth, low birth weight, prenatal exposure to alcohol or tobacco, and early exposure to certain toxins. Importantly, ADHD is not caused by poor parenting, too much screen time, or eating sugar — these are persistent myths. While the environment can affect how symptoms are managed and expressed, the underlying condition is neurodevelopmental.
ADHD frequently co-occurs with other conditions, which can complicate recognition. Common comorbidities include anxiety disorders, depression, learning disorders, and sleep problems. In adults, longstanding undiagnosed ADHD can contribute to anxiety and depression over time, as the accumulated difficulties take a toll on self-esteem and functioning.
Frequently Asked Questions
What is the difference between ADD and ADHD?
ADD (Attention Deficit Disorder) is an older term for what is now called ADHD, predominantly inattentive presentation — attention difficulties without significant hyperactivity. They are not two separate conditions. The term “ADD” was officially used in the DSM-III (1980), but since the DSM-III-R (1987) and especially the DSM-5 (2013), the diagnosis has been consolidated under “Attention-Deficit/Hyperactivity Disorder (ADHD)” with three presentations: predominantly inattentive (what people call ADD), predominantly hyperactive-impulsive, and combined. So when people say “ADD” today, they generally mean inattentive ADHD.
Can you have ADD without hyperactivity?
Yes — that’s precisely what “ADD” refers to. The predominantly inattentive presentation of ADHD involves difficulty with attention, focus, organization, and follow-through, without the prominent restlessness, fidgeting, and impulsivity of the hyperactive-impulsive presentation. This is actually the most common presentation in adults, and it’s frequently underdiagnosed because it’s quiet and doesn’t cause disruptive behavior. It’s especially under-recognized in girls and women, who are more likely to have the inattentive presentation.
What are the 9 symptoms of inattentive ADHD?
The DSM-5 lists nine inattentive symptoms: (1) failing to give close attention to details or making careless mistakes; (2) difficulty sustaining attention in tasks; (3) not seeming to listen when spoken to directly; (4) not following through on instructions and failing to finish tasks; (5) difficulty organizing tasks and activities; (6) avoiding or disliking tasks requiring sustained mental effort; (7) losing things necessary for tasks; (8) being easily distracted; and (9) being forgetful in daily activities. For a diagnosis, adults (17 and older) need at least five of these present for six or more months; children need six. Symptoms must have begun before age 12, occur in more than one setting, and cause significant impairment.
Is ADD a real medical condition?
Yes. While “ADD” itself is an outdated term, the condition it describes — ADHD, inattentive presentation — is a genuine, well-validated neurodevelopmental disorder recognized by the DSM-5-TR, the World Health Organization, and every major medical body. It is one of the most heritable psychiatric conditions (around 74% heritability) and involves measurable differences in brain structure, function, and neurochemistry. ADHD is not a result of laziness, low intelligence, poor parenting, or lack of willpower. It affects roughly 5.9% of children and adolescents and about 3.1% of adults.
Can ADD develop in adults, or do you have to have it as a child?
ADHD is a neurodevelopmental condition that begins in childhood — the DSM-5 requires that several symptoms be present before age 12. However, many people are not diagnosed until adulthood, often because their inattentive symptoms were quiet and went unnoticed, or because they developed coping strategies that masked the difficulties until life demands (college, career, parenthood) overwhelmed them. So while ADHD doesn’t truly “develop” in adulthood, it’s very common to be recognized and diagnosed as an adult. If you suspect you have ADHD as an adult, the childhood-onset requirement means a good evaluation will explore your early history.
What should I do if I score high on this ADD test?
A high score suggests attention difficulties consistent with ADHD, and the recommended next step is a professional evaluation. Start with a healthcare provider — a primary care physician can be an entry point and may refer you to a psychiatrist, psychologist, or ADHD specialist. A proper evaluation includes a thorough history (including childhood), standardized rating scales like the ASRS, and assessment for other conditions that can mimic or accompany ADHD (anxiety, depression, sleep disorders, thyroid issues). ADHD is highly treatable — with medication, CBT adapted for ADHD, skills training, and organizational strategies, all proven effective. This test is a screening tool and cannot diagnose ADHD, but it can be a useful starting point for that conversation.
How accurate is an online ADD test?
An online ADD test is a screening tool, not a diagnostic instrument. It can help you recognize whether your experiences align with ADHD symptoms and decide whether to seek a professional evaluation — but it cannot diagnose ADHD. A formal diagnosis requires a qualified professional to assess the full DSM-5 criteria, including childhood onset (before age 12), presence across multiple settings, significant impairment, and the exclusion of other explanations. This test is informed by DSM-5-TR criteria and the structure of validated screeners like the ASRS, which makes it a meaningful starting point — but the result is a guide for reflection and next steps, not a verdict.
Related Tests
- ADHD Test — the comprehensive companion screen covering all three ADHD presentations (inattentive, hyperactive-impulsive, and combined), designed for adults and based on DSM-5-TR criteria.
- Anxiety Test — anxiety commonly co-occurs with ADHD and can also cause attention difficulties; important to distinguish and assess.
- Clinical Depression Test — depression can impair concentration and frequently co-occurs with ADHD; longstanding, undiagnosed ADHD can also contribute to depression.
- Generalized Anxiety Disorder Test — GAD’s restlessness and difficulty concentrating can overlap with ADHD symptoms; worth differentiating.
- Bipolar Test — bipolar disorder can involve distractibility and impulsivity that overlap with ADHD; the two are sometimes confused or co-occur.
- OCD Test — OCD can affect concentration and is sometimes confused with or co-occurs with ADHD; the underlying mechanisms differ.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Attention-Deficit/Hyperactivity Disorder. psychiatry.org
- Faraone, S.V., et al. (2021). The World Federation of ADHD International Consensus Statement: 208 Evidence-based conclusions about the disorder. Neuroscience & Biobehavioral Reviews, 128, 789–818. [Prevalence ~5.9% youth; heritability ~74%] doi.org
- Matte, B., et al. (2015). ADHD in DSM-5: a field trial in a large, representative sample of 18- to 19-year-old adults. Psychological Medicine, 45(2), 361–373. PMC4301194. [Inattentive symptoms core in adults; DSM-5 thresholds] pmc.ncbi.nlm.nih.gov
- Ayano, G., et al. (2023). The prevalence of adult ADHD: systematic review and meta-analysis. [~3.1% adults; inattentive most common adult presentation] pubmed.ncbi.nlm.nih.gov
- Frontiers in Psychology. (2025). Evaluating attention deficit and hyperactivity disorder (ADHD): a review of current methods and issues. [Terminology history: DSM-II 1968 → DSM-III 1980 ADD subtypes → DSM-5] frontiersin.org
- Kessler, R.C., et al. (2005). The World Health Organization Adult ADHD Self-Report Scale (ASRS). Psychological Medicine, 35(2), 245–256. [Most widely used adult ADHD screener]
- Barkley, R.A. (2010, 2015). Taking Charge of Adult ADHD; Barkley Adult ADHD Rating Scale (BAARS). Guilford Press. [Adult ADHD assessment; family impact]
- Fayyad, J., et al. (2007). Cross-national prevalence and correlates of adult ADHD. British Journal of Psychiatry, 190, 402–409. [Adult prevalence 2.5-3.4%]