
It is not the anger that is the problem. Anger is a normal, human emotion — appropriate and even necessary in the right context. What defines Intermittent Explosive Disorder is a specific pattern: outbursts that are explosive, impulsive, and grossly out of proportion to the situation that triggered them. The reaction doesn’t match the provocation. The intensity cannot be explained by the circumstances. And it happens repeatedly — not as a one-time loss of control but as a recurring pattern that has probably been affecting your life, your relationships, and your sense of who you are for a long time.
People with IED frequently describe the experience in a specific way: a building tension before the outburst, a sudden explosive release, and then — often within minutes — a wave of regret, shame, or embarrassment at what just happened. The outburst felt impossible to stop. It left damage behind. And it almost certainly wasn’t the first time.
This free Intermittent Explosive Disorder Test screens for Intermittent Explosive Disorder (IED) using the DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Based on the past 12 months. Instant, private results.
What Is Intermittent Explosive Disorder?
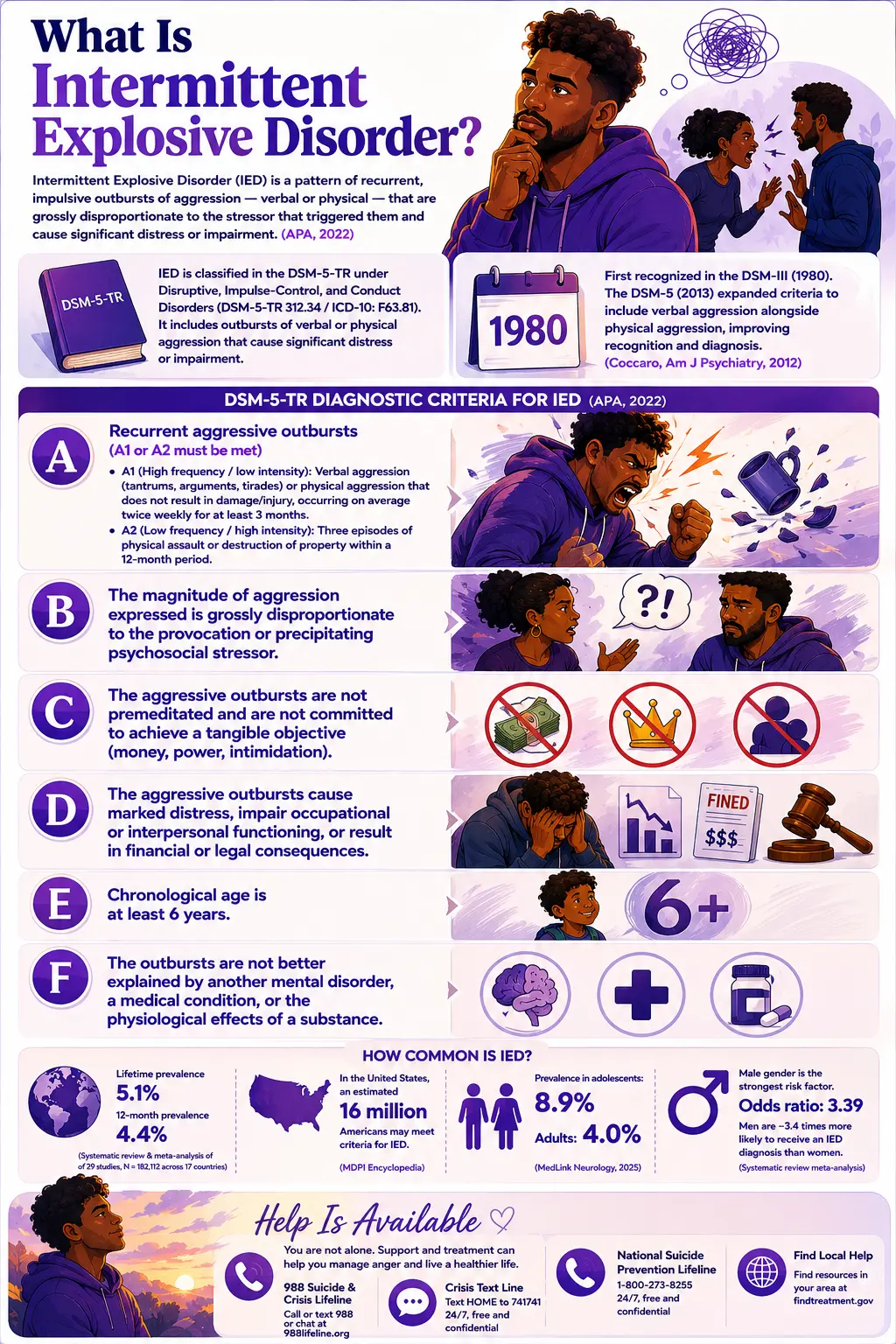
Intermittent Explosive Disorder (IED) is classified under the DSM-5-TR category of Disruptive, Impulse-Control, and Conduct Disorders (DSM-5-TR code 312.34 / ICD-10: F63.81). It is defined as a pattern of recurrent, impulsive, problematic outbursts of aggression — verbal or physical — that are grossly disproportionate to the psychosocial stressor that triggered them and cause significant distress or impairment (APA, 2022).
IED was first formally recognized as a distinct diagnosis in the DSM-III in 1980. A landmark revision in the DSM-5 (2013), driven by research by Dr. Emil F. Coccaro at the University of Chicago — the leading researcher on IED — expanded the diagnostic criteria to include verbal aggression alongside physical aggression, significantly improving the disorder’s clinical recognition (Coccaro, American Journal of Psychiatry, 2012).
The full DSM-5-TR diagnostic criteria for IED (APA, 2022) are:
- Criterion A — Recurrent aggressive outbursts (either A1 or A2 must be met):
A1 (High frequency / low intensity): Verbal aggression (tantrums, verbal arguments, tirades) or physical aggression that does not result in damage to property or physical injury, occurring on average twice weekly for at least 3 months.
A2 (Low frequency / high intensity): Three episodes of physical assault or destruction of property within a 12-month period. - Criterion B: The magnitude of aggression expressed is grossly disproportionate to the provocation or precipitating psychosocial stressor.
- Criterion C: The aggressive outbursts are not premeditated and are not committed to achieve a tangible objective (money, power, intimidation).
- Criterion D: The aggressive outbursts cause marked distress, impair occupational or interpersonal functioning, or result in financial or legal consequences.
- Criterion E: Chronological age is at least 6 years.
- Criterion F: The outbursts are not better explained by another mental disorder, a medical condition, or the physiological effects of a substance.
Although initially thought to be rare, IED is a relatively common and underdiagnosed disorder. A systematic review and meta-analysis of 29 studies (N = 182,112 participants across 17 countries) found a pooled lifetime prevalence of 5.1% and a 12-month prevalence of 4.4%. In the United States specifically, an estimated 16 million Americans may meet the criteria for IED (MDPI Encyclopedia). Prevalence is significantly higher in adolescents — 8.9% of U.S. adolescents meet DSM-5 criteria compared to 4.0% of adults (MedLink Neurology, 2025). Male gender is the strongest demographic risk factor, with an odds ratio of 3.39 — men are approximately 3.4 times more likely to receive an IED diagnosis than women (systematic review meta-analysis).
Signs You Might Have Intermittent Explosive Disorder
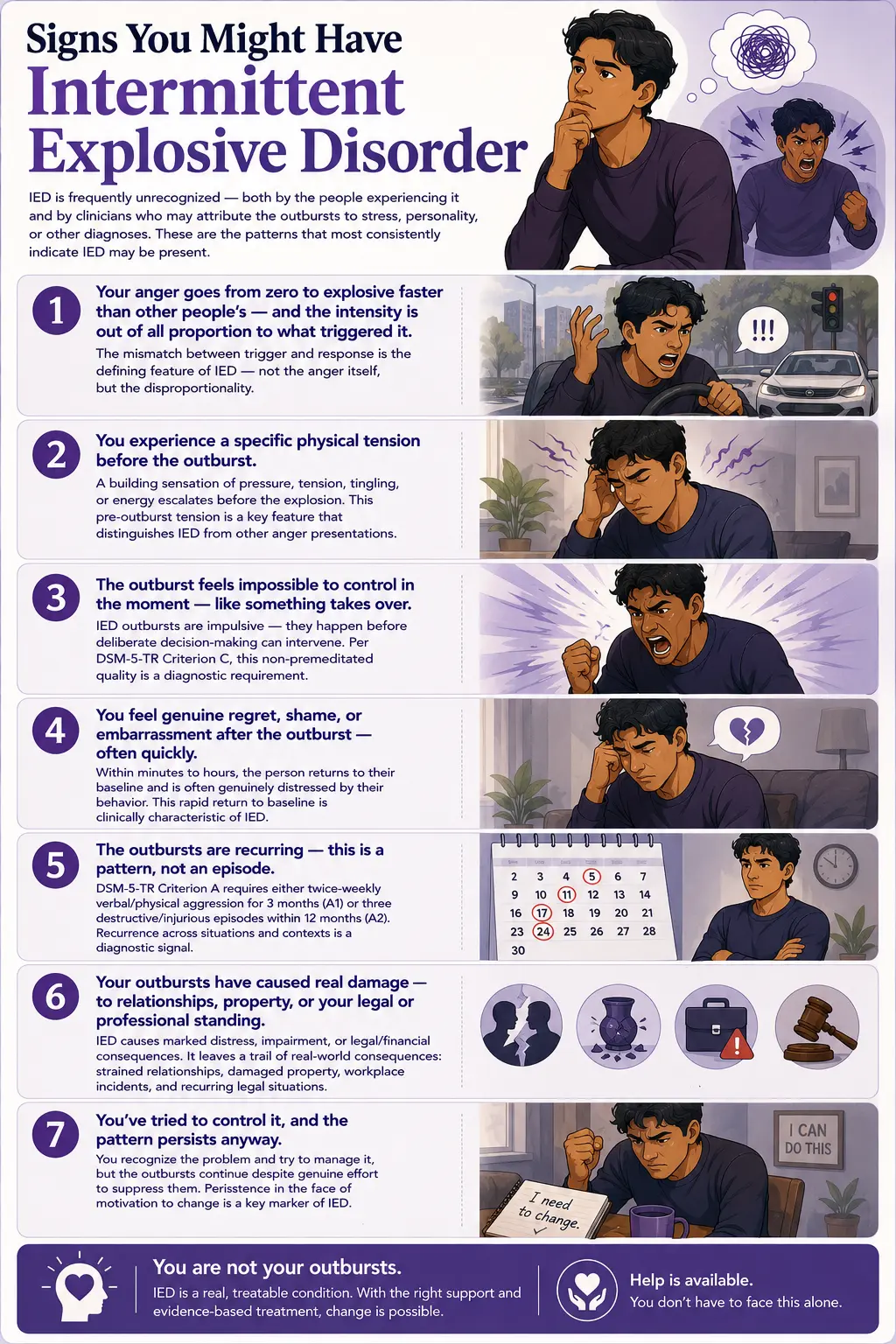
IED is frequently unrecognized — both by the people experiencing it and by clinicians who may attribute the outbursts to stress, personality, or other diagnoses. These are the patterns that most consistently indicate IED may be present:
Your anger goes from zero to explosive faster than other people’s — and the intensity is out of all proportion to what triggered it. Someone cuts you off in traffic and you feel a rage that most people would reserve for a serious personal attack. A minor frustration at home produces an outburst that is more appropriate to a major betrayal. The mismatch between trigger and response is the defining feature of IED — not the anger itself, but the disproportionality.
You experience a specific physical tension before the outburst. Many people with IED describe a characteristic prodrome: a building sensation of pressure, tension, tingling, or energy that escalates before the explosion. This pre-outburst tension is clinically recognized as part of the IED pattern and is one of the features that distinguishes IED from other anger presentations.
The outburst feels impossible to control in the moment — like something takes over. Unlike premeditated aggression, IED outbursts are impulsive — they happen before deliberate decision-making can intervene. The person often describes feeling like they had no choice, or like they were watching themselves from outside. Per DSM-5-TR Criterion C, this non-premeditated quality is a diagnostic requirement.
You feel genuine regret, shame, or embarrassment after the outburst — often quickly. The remorse is frequently rapid and sincere. Within minutes to hours of the outburst, the person returns to their baseline emotional state and is often genuinely distressed by their behavior. This rapid return to baseline — combined with the intensity of the outburst itself — is clinically characteristic of IED.
The outbursts are recurring — this is a pattern, not an episode. A single explosive loss of control under extraordinary circumstances is not an IED. DSM-5-TR Criterion A requires either twice-weekly verbal/physical aggression for 3 months (A1) or three destructive/injurious episodes within 12 months (A2). If this has been happening repeatedly across different situations and different contexts, that recurrence is itself a diagnostic signal.
Your outbursts have caused real damage — to relationships, property, or your legal or professional standing. DSM-5-TR Criterion D requires that the outbursts cause marked distress, functional impairment, or legal/financial consequences. IED is not just a bad temper — it leaves a trail of real-world consequences: strained or broken relationships, damaged property, workplace incidents, and legal situations that keep arising from the same uncontrollable pattern.
You’ve tried to control it, and the pattern persists anyway. People with IED are often not indifferent to the problem — they frequently recognize the pattern, feel ashamed of it, and try to manage it. What defines IED is that the outbursts continue despite genuine effort to suppress them. The persistence in the face of motivation to change is one of the clearest markers of a clinical condition rather than a behavioral choice.
IED vs Normal Anger vs BPD vs ASPD — The Critical Distinctions
IED is frequently confused with other conditions and with normal anger. Understanding the distinctions is clinically important because they determine the appropriate treatment approach.
| Feature | Normal Anger | IED | Borderline PD (BPD) | Antisocial PD (ASPD) |
|---|---|---|---|---|
| Nature of aggression | Proportionate to the provocation; subsides with resolution | Grossly disproportionate; impulsive; non-premeditated | Impulsive; often triggered by abandonment fears or identity disturbance | May be calculated and premeditated; used as a tool |
| Premeditation | Not applicable | None — DSM Criterion C requires non-premeditated | Typically impulsive but embedded in broader emotional dysregulation | Often deliberate and goal-directed |
| Post-outburst response | Proportionate; may still feel the anger was justified | Rapid return to baseline; often genuine remorse and shame | Emotional dysregulation persists; more sustained distress | Little remorse; may justify behavior |
| Broader personality features | None | Outbursts are episodic; personality between episodes is generally unremarkable | Pervasive identity disturbance, chronic emptiness, fear of abandonment | Disregard for rules and others’ rights; deceitfulness; lack of empathy |
| DSM-5-TR classification | Not a disorder | Disruptive, Impulse-Control, and Conduct Disorders (312.34) | Cluster B Personality Disorder (301.83) | Cluster B Personality Disorder (301.7) |
| PsyMed test | No test needed | This test | BPD Test | ASPD Test |
An important clinical note on IED and BPD: both involve impulsive aggression and can present very similarly. The key distinction is scope — IED is characterized by episodic outbursts with relatively unremarkable personality functioning between episodes, while BPD involves pervasive emotional dysregulation, chronic identity disturbance, and a broader pattern of interpersonal difficulty that extends well beyond the angry episodes. Both can and do co-occur; the presence of IED does not rule out BPD.
What Causes Intermittent Explosive Disorder?
IED develops from an interaction of neurobiological, genetic, and environmental factors. The leading research on IED etiology comes from Dr. Emil F. Coccaro’s laboratory at the University of Chicago, which has produced the most comprehensive body of work on IED’s underlying mechanisms.
Serotonin system dysfunction. Neurobiological research has consistently identified reduced central serotonergic (5-HT) function as a core biological feature of IED (MedLink Neurology, 2025). Serotonin plays a key role in impulse control, mood regulation, and the inhibition of aggressive responses. Reduced 5-HT function appears to lower the threshold at which provocation triggers an aggressive response, contributing to the characteristic disproportionality of IED outbursts.
Frontal-limbic dysregulation. Neuroimaging research has identified reduced frontal-limbic grey matter and enhanced amygdala response to social threat in individuals with IED (MedLink Neurology, 2025). The amygdala drives the threat-detection and emotional reactivity response; the frontal cortex regulates and inhibits that response. In IED, the balance appears to tip toward heightened reactivity and reduced inhibition.
Hostile attribution bias. A core cognitive feature of IED is the tendency to interpret ambiguous social situations as hostile or threatening — reading neutral facial expressions as angry, interpreting accidental provocations as intentional, and assuming malicious intent in ambiguous interactions (MedLink Neurology, 2025). This bias means the person with IED is effectively operating in a social environment that feels more threatening than it actually is.
Genetic factors. IED shows significant familial aggregation — it runs in families. Studies by Coccaro and colleagues have documented a family history of impulsive aggression or related disorders as a consistent risk factor, suggesting both genetic transmission of serotonergic vulnerability and environmental modeling of explosive behavior patterns.
Childhood trauma and adverse experiences. Exposure to physical or emotional trauma, particularly during childhood, significantly increases IED risk. ScienceDirect (2018) notes that IED is uniquely associated with both a history of childhood abuse and a diagnosis of alcohol use disorder. The systematic review meta-analysis confirmed trauma exposure as a robust risk factor for IED across 17 countries.
Comorbidities. IED has significant comorbidity with mood disorders, anxiety disorders, substance use disorders, and ADHD. The systematic review meta-analysis identified mood disorders, anxiety disorders, and substance use disorders as the most robust psychiatric comorbidity risk factors.
How This Intermittent Explosive Disorder Test Works
This IED test screens for Intermittent Explosive Disorder using the DSM-5-TR diagnostic framework (APA, 2022), drawing on the IED Screening Questionnaire (IED-SQ) developed by Coccaro and colleagues (2017) and published in the research literature. It covers both Criterion A1 (high-frequency/low-intensity) and Criterion A2 (low-frequency/high-intensity) outburst patterns, the disproportionality requirement (Criterion B), the non-premeditated quality (Criterion C), and the functional impact (Criterion D) across 15 questions.
Answer based on your consistent experience over the past 12 months — not a single episode, but the recurring pattern.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. This is a screening tool — it cannot diagnose IED. Only a qualified mental health professional can diagnose a disorder through a comprehensive clinical assessment.
Understanding Your IED Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few IED Indicators | Responses suggest few significant IED patterns. Anger management concerns may be present without a pattern consistent with Intermittent Explosive Disorder. |
| 16 – 30 | Mild — Some IED Patterns Present | Some explosive anger patterns present. May not reach full IED threshold but warrants professional discussion and anger management support. |
| 31 – 45 | Moderate — Significant IED Pattern | A significant pattern of explosive, disproportionate anger across multiple domains. Consistent with IED; professional evaluation is recommended. |
| 46 – 60 | High — Strong IED Indicators | Pervasive and severe explosive anger patterns. Professional evaluation and treatment are strongly recommended. |
Treatment for Intermittent Explosive Disorder
Cognitive Behavioral Therapy (CBT). The most evidence-supported psychological treatment for IED. CBT for IED targets three specific mechanisms: (1) cognitive restructuring of hostile attribution bias — the tendency to read ambiguous situations as threatening; (2) relaxation and arousal reduction techniques applied to interrupt the pre-outburst tension escalation; (3) behavioral skills to create a pause between the provocation and the explosive response. Group CBT formats have demonstrated particular efficacy for IED, providing both the skills training and the social learning context that the disorder specifically requires.
Pharmacotherapy — SSRIs. Fluoxetine has demonstrated efficacy in randomized controlled trials for IED (Coccaro and colleagues), with significant reductions in aggressive outburst frequency and intensity. The proposed mechanism is restoration of central serotonergic function — the neurobiological deficit most consistently identified in IED research. SSRIs are typically used alongside rather than instead of CBT.
Dialectical Behavior Therapy (DBT). DBT — originally developed by Dr. Marsha Linehan for BPD — has applicability to IED given its specific focus on emotional regulation, distress tolerance, and impulse control. For individuals with comorbid IED and BPD or significant emotional dysregulation, DBT may be the more appropriate primary therapeutic framework.
Frequently Asked Questions
What is Intermittent Explosive Disorder?
Intermittent Explosive Disorder (IED) is a Disruptive, Impulse-Control, and Conduct Disorder (DSM-5-TR 312.34 / F63.81) characterized by recurrent, impulsive, disproportionate aggressive outbursts — verbal or physical — that are not premeditated and cause significant distress or functional consequences. Diagnosis requires either twice-weekly verbal/physical aggression for 3+ months (Criterion A1) or three destructive/injurious episodes within 12 months (Criterion A2), plus the outbursts must be grossly disproportionate to the provocation, non-premeditated, and not better explained by another condition. IED affects approximately 5% of the general population, with an estimated 16 million Americans meeting criteria, and is significantly more prevalent in adolescents (8.9%) than adults (4.0%).
Is IED just a bad temper?
No — the distinction is important clinically. A bad temper refers to a general tendency toward irritability, frustration, or anger that may be proportionate or only somewhat exaggerated. IED is defined by a specific pattern: outbursts that are grossly disproportionate to the provocation, impulsive rather than premeditated, recurring rather than isolated, and causing real functional consequences. DSM-5-TR Criterion B explicitly requires the disproportionality. Someone with a bad temper may be consistently irritable and difficult; someone with IED experiences discrete explosive episodes that they often describe as feeling out of their control, followed by a rapid return to baseline and genuine remorse.
How is IED different from bipolar disorder?
In bipolar disorder, irritability and aggression occur within the context of distinct mood episodes — manic, hypomanic, or mixed — and are accompanied by other features of the mood episode (elevated mood, reduced sleep, grandiosity, racing thoughts, increased goal-directed activity). In IED, the explosive episodes are discrete outbursts without the broader mood state changes that characterize bipolar episodes. The person with IED returns to their normal baseline between outbursts, rather than cycling through sustained mood states. Both can co-occur, and the presence of IED does not rule out bipolar disorder. The Bipolar Test is worth completing if mood cycling is also present.
Can IED affect teenagers?
Yes — IED is actually more prevalent in adolescents than adults. MedLink Neurology (2025) reports that 8.9% of U.S. adolescents meet DSM-5 criteria for IED compared to 4.0% of adults. DSM-5-TR Criterion E specifies a minimum age of 6 years, recognizing that IED does occur in children and adolescents. The GSC data for this page shows active searches for “IED test for teens,” reflecting real need for this assessment in younger populations. For adolescents, the approach to treatment may emphasize family involvement and school coordination alongside individual CBT.
What is the relationship between IED and trauma?
Research consistently links IED with a history of childhood trauma, abuse, and adverse experiences. ScienceDirect (2018) notes that IED is uniquely associated with both a history of childhood abuse and a diagnosis of alcohol use disorder relative to healthy and psychiatric comparison groups. The systematic review meta-analysis confirmed trauma exposure as a robust risk factor across 17 countries. However, the relationship is complex: trauma increases the risk of developing IED but does not cause it directly, and not everyone with IED has a trauma history. Where trauma and IED co-occur, PTSD assessment and trauma-informed treatment approaches are important components of the treatment plan.
Can IED be treated?
Yes — IED is a treatable condition with meaningful reduction in outburst frequency and intensity achievable through appropriate intervention. CBT focused on hostile attribution restructuring and arousal management is the most evidence-supported psychological treatment. SSRIs — particularly fluoxetine — have demonstrated efficacy in randomized controlled trials in reducing aggressive behavior in IED (Coccaro and colleagues). A combination of CBT and medication produces the strongest outcomes. The neurobiological basis of IED (serotonin dysfunction, amygdala hyperreactivity) means that treatment is not simply about willpower or behavioral modification — it addresses the underlying neurological mechanisms that drive the pattern.
How does IED affect relationships?
IED typically produces cumulative damage to relationships over time. The outbursts — whether verbal or physical — leave psychological traces even when the person with IED feels genuine remorse afterward. Partners, family members, and colleagues often become hypervigilant about the person’s emotional state, walking on eggshells to avoid triggering an episode. This chronic tension changes the nature of relationships in ways that persist between outbursts. Relationship problems, workplace difficulties, and legal difficulties are specifically listed in the research as consequences associated with IED (ScienceDirect, 2018). Couples therapy or family therapy as a complement to individual IED treatment is often clinically indicated.
Related Tests
- Multidimensional Anger Test — the most important companion test; covers the full dimensions of anger, including anger-in, anger-out, and anger control — complementary to the IED-specific screening
- Borderline Personality Disorder Test — BPD and IED share impulsive aggression and can co-occur; the broader personality pattern needs assessment
- Antisocial Personality Disorder Test — ASPD involves aggression that is more premeditated and goal-directed, contrasting with IED’s impulsive, non-premeditated pattern
- Bipolar Test — bipolar disorder, especially mixed episodes, can produce explosive irritability that overlaps with IED presentations
- ADHD Test — ADHD and IED frequently co-occur; impulsivity in ADHD can contribute to the explosive pattern, and both need to be addressed
- Anxiety Test — anxiety disorders are among the most common IED comorbidities; chronic anxiety increases arousal and lowers the threshold for explosive responses
- Clinical Depression Test — mood disorders are documented IED comorbidities and need separate assessment and treatment
- PTSD Test — trauma history is a robust IED risk factor; PTSD and IED frequently co-occur and require integrated treatment
- Passive-Aggressive Test — some individuals alternate between explosive expression and passive-aggressive patterns; worth assessing alongside IED
For more impulse control and addiction assessments, visit our Addiction and Impulse Control collection.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Intermittent Explosive Disorder 312.34 (F63.81). psychiatry.org
- Coccaro, E.F. (2012). Intermittent Explosive Disorder as a Disorder of Impulsive Aggression for DSM-5. American Journal of Psychiatry, 169(6), 577–588. pubmed.ncbi.nlm.nih.gov
- Coccaro, E.F., Lee, R., & McCloskey, M.S. (2014). Validity of the new A1 and A2 criteria for DSM-5 Intermittent Explosive Disorder. Comprehensive Psychiatry, 55(2), 260–267. sciencedirect.com
- Rynar, L., & Coccaro, E.F. (2018). Psychosocial impairment in DSM-5 Intermittent Explosive Disorder. Psychiatry Research, 264, 91–95. sciencedirect.com
- Kessler, R.C., et al. (2006). The prevalence and correlates of DSM-IV intermittent explosive disorder in the National Comorbidity Survey Replication. Archives of General Psychiatry, 63(6), 669–678. [5.4% lifetime prevalence, USA]
- MedLink Neurology. (2025). Intermittent Explosive Disorder. medlink.com
- MDPI Encyclopedia. (2022). Intermittent Explosive Disorder. [16 million Americans] encyclopedia.pub
- Systematic Review & Meta-Analysis. (2024). Angry Without Borders: Global prevalence and factors of Intermittent Explosive Disorder. [29 studies, N=182,112, lifetime 5.1%]
- Burke, J.D., et al. (2024). Evidence-Based Assessment of DSM-5 Disruptive, Impulse Control, and Conduct Disorders. Psychological Assessment. sagepub.com
- Wikipedia. (2025). Intermittent explosive disorder. en.wikipedia.org