It’s not the kind of low that knocks you down dramatically. It’s quieter than that. A persistent flatness — a mood that doesn’t fully lift, a tiredness that doesn’t fully resolve, a sense of going through the motions that has lasted so long it has started to feel like just who you are.
That is what dysthymia — now formally classified as Persistent Depressive Disorder — looks like from the inside. Not a breakdown. Not a crisis. Just a chronic, low-grade heaviness that has become the background of your life. And because it’s not acute, many people carry it for years before anyone — including themselves — recognizes it as something worth treating.
This free Dysthymia Test screens for the patterns associated with Persistent Depressive Disorder (PDD) using DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Based on your experience over the past 2 years. Results are instant and private.
What Is Dysthymia?
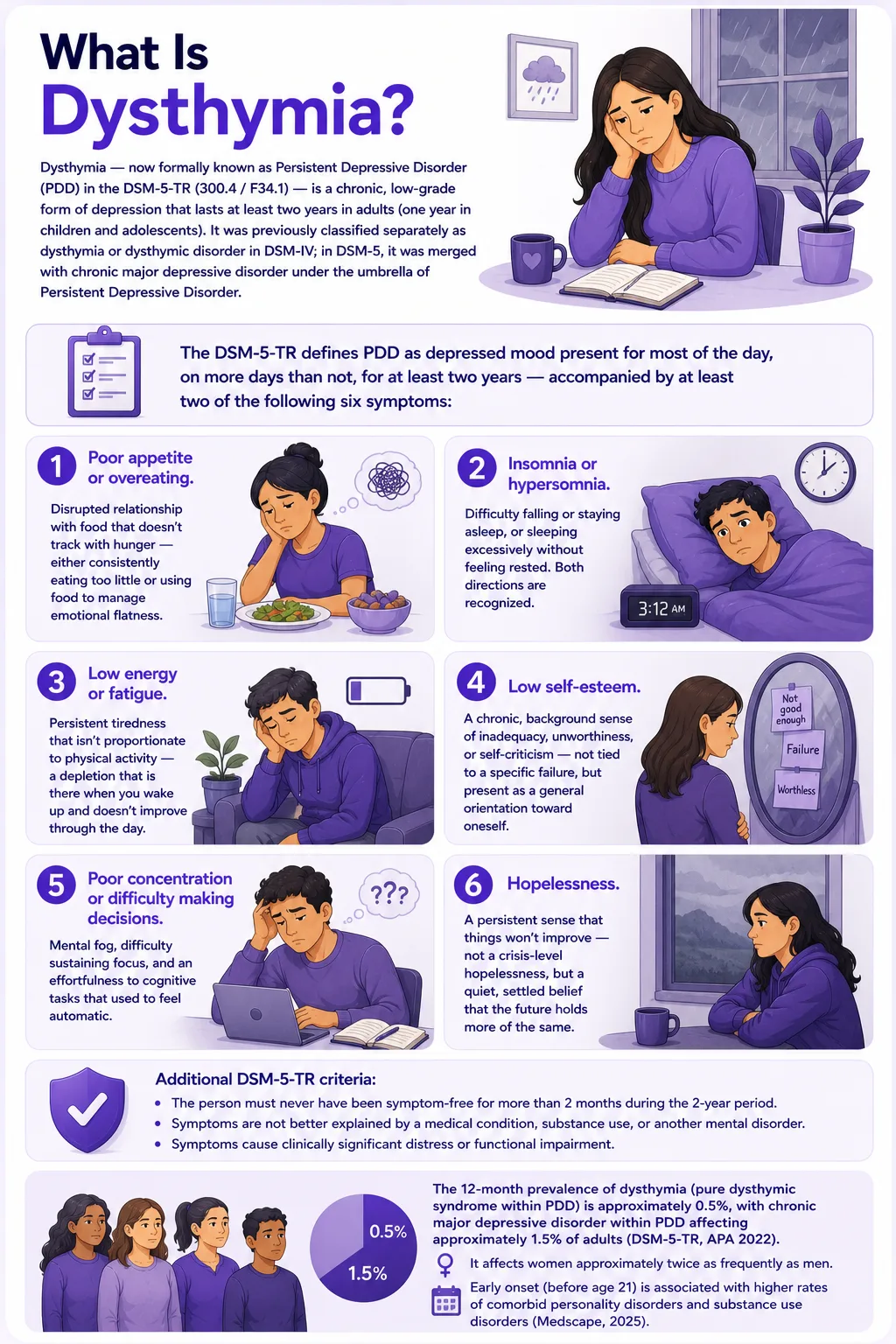
Dysthymia — now formally known as Persistent Depressive Disorder (PDD) in the DSM-5-TR (300.4 / F34.1) — is a chronic, low-grade form of depression that lasts at least two years in adults (one year in children and adolescents). It was previously classified separately as dysthymia or dysthymic disorder in DSM-IV; in DSM-5, it was merged with chronic major depressive disorder under the umbrella of Persistent Depressive Disorder.
The DSM-5-TR defines PDD as depressed mood present for most of the day, on more days than not, for at least two years — accompanied by at least two of the following six symptoms:
- Poor appetite or overeating. Disrupted relationship with food that doesn’t track with hunger — either consistently eating too little or using food to manage emotional flatness.
- Insomnia or hypersomnia. Difficulty falling or staying asleep, or sleeping excessively without feeling rested. Both directions are recognized.
- Low energy or fatigue. Persistent tiredness that isn’t proportionate to physical activity — a depletion that is there when you wake up and doesn’t improve through the day.
- Low self-esteem. A chronic, background sense of inadequacy, unworthiness, or self-criticism — not tied to a specific failure, but present as a general orientation toward oneself.
- Poor concentration or difficulty making decisions. Mental fog, difficulty sustaining focus, and an effortfulness to cognitive tasks that used to feel automatic.
- Hopelessness. A persistent sense that things won’t improve — not a crisis-level hopelessness, but a quiet, settled belief that the future holds more of the same.
Additional DSM-5-TR criteria: the person must never have been symptom-free for more than 2 months during the 2-year period; symptoms are not better explained by a medical condition, substance use, or another mental disorder; and symptoms cause clinically significant distress or functional impairment.
The 12-month prevalence of dysthymia (pure dysthymic syndrome within PDD) is approximately 0.5%, with chronic major depressive disorder within PDD affecting approximately 1.5% of adults (DSM-5-TR, APA 2022). It affects women approximately twice as frequently as men. Early onset (before age 21) is associated with higher rates of comorbid personality disorders and substance use disorders (Medscape, 2025).
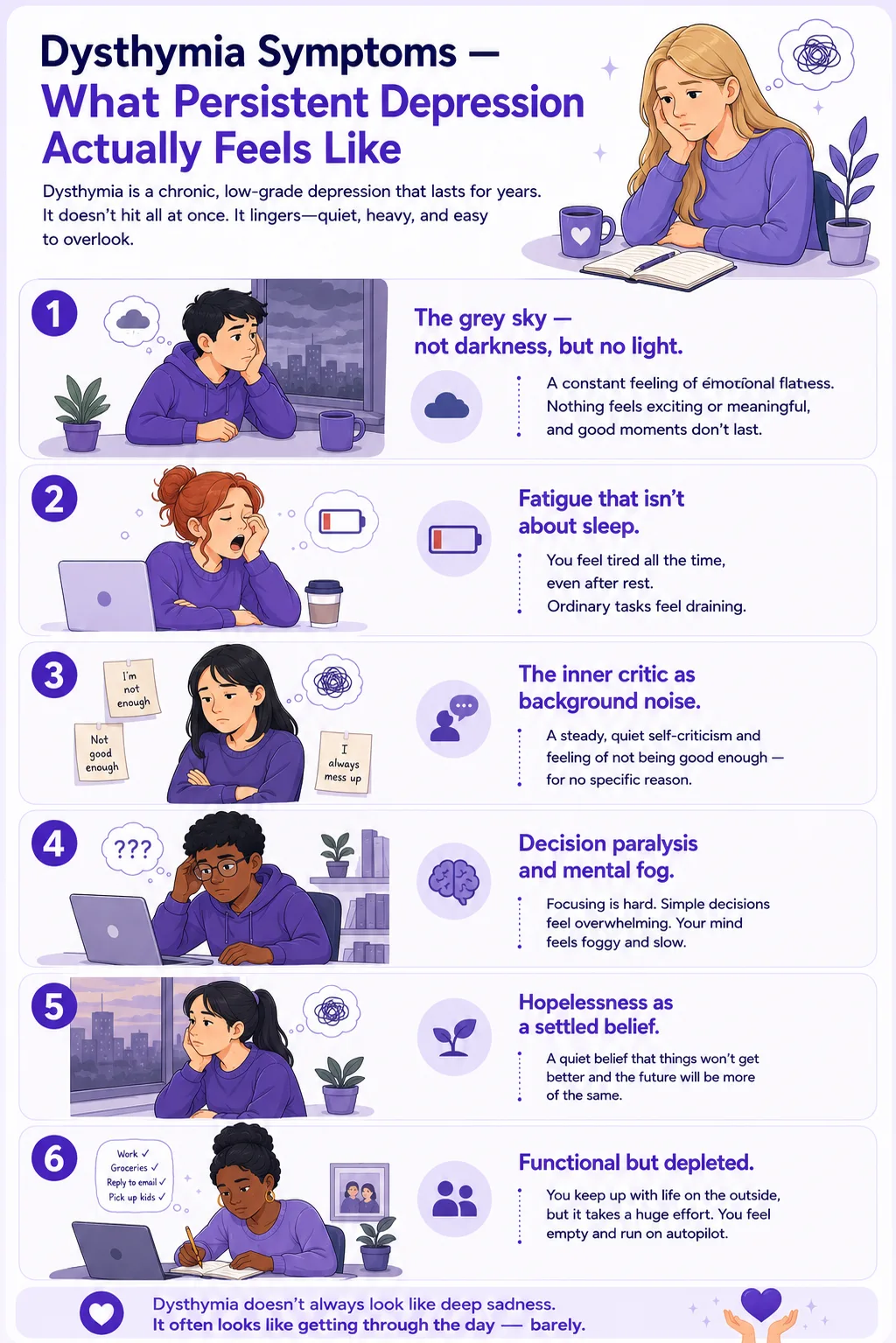
Dysthymia Symptoms — What Persistent Depression Actually Feels Like
Because dysthymia doesn’t produce the dramatic low of a major depressive episode, it is frequently unrecognized by the person experiencing it and by the people around them. Many people with PDD describe having “always been this way” — interpreting a chronic mood disorder as a personality trait. This is one of the most clinically significant features of dysthymia and one of the main reasons it goes untreated for years.
The grey sky — not darkness, but no light. The hallmark of dysthymia is not acute sadness but a persistent emotional flatness. Not depression’s characteristic absence of pleasure in specific things, but a pervasive dimness — the world lacks color, experiences don’t land fully, and positive moments don’t accumulate into a sense of well-being. It’s more like being three feet behind yourself than being in pain.
Fatigue that isn’t about sleep. People with dysthymia often describe being exhausted by ordinary tasks — not because of exertion, but because the basic effort of existing in their mood state is draining. Sleep, when it comes, doesn’t restore. Mornings are often the hardest part of the day.
The inner critic as background noise. Low self-esteem in dysthymia often presents not as dramatic self-loathing but as a steady, quiet stream of self-critical commentary — a default assumption of inadequacy that doesn’t require a specific trigger. Many people don’t experience this as low self-esteem; they experience it as realistic self-assessment.
Decision paralysis and mental fog. Concentration difficulties in dysthymia tend to be subtle — not an inability to think, but an effortfulness to cognitive tasks that weren’t always effortful. Making decisions feels disproportionately hard. The mental energy required to process and choose feels depleted before the decision is made.
Hopelessness as a settled belief. The hopelessness of dysthymia is characteristically quiet — not a crisis of despair, but a stable background assumption that things are unlikely to improve significantly. This often manifests as a lack of investment in future planning, difficulty imagining substantial change, and a subtle resistance to treatment (because improvement doesn’t feel genuinely possible).
Functional but depleted. People with dysthymia often continue to function — going to work, maintaining relationships, fulfilling responsibilities. This is one of the reasons dysthymia goes unrecognized. From the outside, and sometimes even from the inside, nothing looks dramatically wrong. But the internal cost of that functioning — the effort required, the absence of enjoyment, the sense of running on empty — is real and significant.
Dysthymia vs. Major Depression vs. “Just Sadness” — The Key Distinctions
One of the most important clinical distinctions for anyone questioning whether what they’re experiencing is dysthymia is understanding how it differs from both major depression and normal fluctuations in mood.
| Feature | Normal Sadness | Dysthymia (PDD) | Major Depressive Disorder |
|---|---|---|---|
| Duration | Days to weeks — proportionate to circumstances | 2+ years continuous (no more than 2 months symptom-free) | Episodes lasting 2+ weeks; may resolve between episodes |
| Severity | Mild, resolves naturally | Mild to moderate — persistent, not episodic | Moderate to severe — often acutely impairing |
| Mood pattern | Reactive to circumstances, improves with positive events | Chronic baseline low — doesn’t fully lift with positive events | Episodic, may have periods of normal mood between episodes |
| Onset recognition | Clear trigger, clear start | Often insidious — “I’ve always been this way.” | Often a discernible onset from the previous baseline |
| Functional impact | Minimal | Significant — effortful functioning, not acute impairment | Often severe — work, relationships, and daily tasks are significantly impaired |
| Double depression | N/A | Can co-occur with MDD episodes (“double depression”) | Can occur on top of PDD baseline — most severe combination |
| PsyMed screening | No screening needed | This test | Clinical Depression Test |
Double depression — the simultaneous occurrence of PDD and a major depressive episode — is a clinically important pattern. Research suggests that up to 75% of people with dysthymia will experience at least one major depressive episode during their lifetime (Kocsis & Klein, 1995). When a major depressive episode occurs on top of a dysthymia baseline, the combined presentation tends to be more severe and harder to treat than either condition alone.
What Causes Persistent Depressive Disorder?
PDD develops from the interaction of genetic predisposition, neurobiological factors, psychological patterns, and life experience. The current research understanding is that dysthymia shares much of the same etiology as major depression, but with specific contributors to chronicity.
Genetic and familial factors
PDD has significant heritability. First-degree relatives of people with PDD are at elevated risk for both PDD and major depressive disorder. Research suggests that individuals with PDD are more likely to have first-degree relatives with PDD specifically than with episodic MDD — suggesting some distinct genetic contribution to the chronicity dimension (DSM-5, APA 2013).
Neurobiological factors
The serotonin transporter gene polymorphism has been studied in relation to PDD, with research suggesting interactions between genetic variants and early adverse experiences in promoting depressive chronicity (Psychiatric Times, 2025). Dysregulation in the HPA (hypothalamic-pituitary-adrenal) axis — the brain’s stress response system — is consistently associated with chronic depression and is thought to contribute to its persistence.
Early onset and childhood adversity
Early onset PDD (before age 21) is specifically associated with childhood maltreatment, adverse childhood experiences, and early relational disruptions. Strong associations between childhood maltreatment and depressive chronicity are among the most replicated findings in PDD research (Psychiatric Times, 2025). Children who develop PDD often grow up experiencing their depressive symptoms as personality rather than a disorder.
Psychological patterns
Cognitive patterns associated with dysthymia include negative schemas about self, world, and future — the cognitive triad first described by Beck (1979) in the context of depression. In PDD, these schemas are often highly stable and ego-syntonic (they feel like accurate assessments rather than distorted thinking), which is why people with dysthymia often don’t seek help and often resist the idea that their mood is treatable.
Comorbid conditions
PDD has high rates of comorbidity with anxiety disorders, major depressive disorder, substance use disorders, and personality disorders — particularly in early-onset presentations. It is also frequently comorbid with chronic medical conditions, which both contribute to and are worsened by persistent depression. Comorbid ADHD is increasingly recognized as a contributor to concentration difficulties in PDD.
How This Dysthymia Test Works
This test screens for Persistent Depressive Disorder using the DSM-5-TR diagnostic criteria for PDD (APA, 2022) — the six core symptom domains plus the chronic mood pattern and functional impact that define it. All 15 questions assess your experience over the past 2 years, not just recent weeks, because the 2-year duration criterion is what distinguishes dysthymia from a depressive episode.
Answer based on your consistent, typical experience over this period — not your best period, and not your worst episode. The scale is:
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Total range: 0–60. This is a screening tool — it cannot diagnose PDD. A significant score is clinically meaningful and warrants a visit to a healthcare provider for proper evaluation.
Understanding Your Dysthymia Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few PDD Indicators | Responses suggest a few significant, persistent depressive symptoms. Normal mood fluctuations may be present without a pattern consistent with PDD. |
| 16 – 30 | Mild — Some Persistent Depressive Patterns | Some persistent depressive symptom patterns are present. These may not reach full PDD criteria, but are worth monitoring and discussing with a professional if they persist. |
| 31 – 45 | Moderate — Significant PDD Pattern | A significant pattern of persistent depressive symptoms is present across multiple domains. This is consistent with PDD and warrants professional evaluation. |
| 46 – 60 | High — Strong PDD Indicators | Strong and pervasive persistent depressive patterns are indicated across most domains. Professional evaluation and support are strongly recommended. |
Treatment for Persistent Depressive Disorder — What Works
PDD has historically been considered harder to treat than episodic depression, with lower remission rates and longer treatment timelines. But the clinical evidence for effective treatment is substantial, and the understanding of why PDD is harder to treat has improved significantly, which has informed better treatment approaches.
Cognitive Behavioral Analysis System of Psychotherapy (CBASP)
The only psychotherapy specifically designed for chronic depression. CBASP targets the interpersonal patterns and cognitive styles that maintain chronicity — particularly the disconnection between behavior and consequences that is characteristic of chronic depression. It has shown efficacy in randomized controlled trials specifically for PDD and chronic depression populations.
Cognitive Behavioral Therapy (CBT)
The most broadly evidenced psychotherapy for depression. CBT for PDD targets the stable negative schemas about self, world, and future that are characteristic of the condition — with particular attention to the ego-syntonic nature of those schemas (the fact that they feel like accurate beliefs rather than distorted ones). CBT for PDD typically requires a longer duration than for episodic depression.
Interpersonal Therapy (IPT)
Focuses on the relationship between current interpersonal patterns and mood. Dr. John Markowitz at Columbia University has been among the leading researchers in applying IPT specifically to dysthymia and chronic depression, with evidence showing its effectiveness particularly for interpersonal difficulties that maintain the chronic pattern.
SSRIs and SNRIs
Sertraline has the strongest evidence base for PDD specifically among SSRIs. Venlafaxine and duloxetine (SNRIs) are also commonly used. Medication for PDD typically needs to be continued longer than for episodic depression to prevent relapse, and treatment duration is usually measured in years rather than months for those with early-onset or long-standing presentations.
Combined treatment
Research consistently shows that combined pharmacotherapy and psychotherapy produce superior outcomes to either alone for PDD — particularly for moderate-to-severe and long-duration presentations (Psychiatric Times, 2025). This is the standard recommendation for most clinical presentations of PDD.
Frequently Asked Questions
What is dysthymia?
Dysthymia is the former name for what is now classified as Persistent Depressive Disorder (PDD) in the DSM-5-TR (300.4 / F34.1). It is a chronic, low-grade form of depression lasting at least two years in adults, characterized by depressed mood on most days plus at least two of six symptoms: poor appetite or overeating, insomnia or hypersomnia, low energy or fatigue, low self-esteem, poor concentration or difficulty making decisions, and hopelessness. Unlike major depressive disorder, PDD is not episodic — it is a continuous pattern without significant symptom-free periods. It affects approximately 1–4% of adults in the general population.
What is the difference between dysthymia and depression?
Both dysthymia (PDD) and major depressive disorder (MDD) are depressive conditions, but they differ primarily in duration, severity, and pattern. MDD is episodic — occurring in discrete episodes, typically more severe, with periods of normal mood between them. Dysthymia is chronic and lower-grade — present more days than not for at least two years, without the dramatic low of a major depressive episode. The key clinical distinction is that dysthymia is the chronic baseline, while MDD is the acute episode. They can co-occur as “double depression,” which is the most severe and difficult-to-treat combination. Our Clinical Depression Test screens specifically for major depressive disorder.
How do I know if I have dysthymia or just feel sad?
The key distinguishing features are duration, pervasiveness, and functional impact. Normal sadness is proportionate to circumstances, resolves within days to weeks, and doesn’t significantly impair daily functioning. Dysthymia is present on most days for at least two years, doesn’t lift fully even when circumstances improve, and creates a consistent drag on energy, self-perception, concentration, and hope. Many people with dysthymia describe not having a clear “before” — the low has been present so long they’ve stopped identifying it as a departure from their baseline. If you can’t remember the last extended period when you felt genuinely well — not just functional, but actually well — that duration pattern is clinically significant.
Can dysthymia go away on its own?
Sometimes, though, the research evidence suggests that untreated PDD tends to follow a chronic course — and that the average duration before treatment is typically measured in years. The chronicity itself is partly maintained by the hopelessness that is a symptom of the condition (the belief that things won’t improve discourages help-seeking). With treatment, outcomes are meaningfully better — particularly with combined therapy and medication. The earlier the treatment is started, the better the long-term outcome, both in terms of remission and in reducing the risk of developing comorbid major depressive episodes.
What is “double depression”?
Double depression refers to the occurrence of a major depressive episode on top of a pre-existing Persistent Depressive Disorder baseline. Research suggests that up to 75% of people with dysthymia will experience at least one major depressive episode during their lifetime. When double depression occurs, it presents as a distinct, more acute worsening of symptoms against the chronic background. It is clinically important to identify because treatment needs to address both the acute episode and the underlying chronic condition — treating only the episode without addressing the PDD baseline typically results in return to the chronic low rather than full recovery.
Is dysthymia related to burnout or depression?
Dysthymia, burnout, and major depression share significant symptom overlap — fatigue, low motivation, difficulty concentrating, emotional depletion — and they can co-occur. The key distinctions: burnout is specifically linked to chronic occupational stress and typically improves with rest and reduced stress; major depression is episodic and more acutely severe; dysthymia is chronic and lower-grade, often present regardless of stress levels, and doesn’t resolve with rest alone. Our Burnout Test is worth completing if work-related stress is a significant factor, as the distinction meaningfully affects the treatment approach.
Related Tests
Dysthymia rarely exists in isolation. These tests cover the conditions most commonly associated with it or confused with it:
- Clinical Depression Test — screens for major depressive disorder; essential if you suspect a more severe or episodic depression on top of a chronic baseline
- Anxiety Test — anxiety disorders are the most common comorbidity with PDD; they very frequently co-occur and affect the treatment approach
- Burnout Test — shares significant symptom overlap with dysthymia; important to distinguish, as the treatment approaches differ
- Bipolar Test — persistent low mood with occasional elevated periods may indicate a bipolar spectrum condition rather than PDD; important to rule out before treatment
- ADHD Test — concentration difficulties and low motivation in dysthymia overlap significantly with ADHD; both conditions frequently co-occur
- Anhedonia Test — loss of pleasure and emotional flatness are core features of PDD; this test explores that dimension specifically
- PTSD Test — childhood adversity and trauma are among the strongest risk factors for PDD; PTSD and PDD frequently co-occur in people with early trauma histories
- Edinburgh Postnatal Depression Scale (EPDS) — dysthymia is a significant risk factor for perinatal depression; if you are pregnant or have recently given birth, the EPDS is the validated screening tool for this period
For more mood and depression screenings, visit our Mood and Depression collection.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Persistent Depressive Disorder 300.4 (F34.1). psychiatry.org
- Patel, R.K., & Rose, G.M. (2024). Persistent Depressive Disorder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. ncbi.nlm.nih.gov
- Psychiatric Times. (2025). Persistent Depressive Disorder, Dysthymia, and Chronic Depression: Update on Diagnosis, Treatment. psychiatrictimes.com
- Medscape. (2025). Dysthymic Disorder: Background, Etiology, Epidemiology. emedicine.medscape.com
- Cleveland Clinic. (2024). Persistent Depressive Disorder (PDD): Symptoms & Treatment. my.clevelandclinic.org
- Kocsis, J.H., & Klein, D.N. (Eds.). (1995). Diagnosis and Treatment of Chronic Depression. Guilford Press.
- Akiskal, H.S. (2001). Dysthymia and cyclothymia in psychiatric practice a century after Kraepelin. Journal of Affective Disorders, 62(1–2), 17–31. PMID: 11172668
- Uher, R., et al. (2012). Persistent depressive disorder: A review. Current Psychiatry Reports. pmc.ncbi.nlm.nih.gov