
A panic attack is one of the most frightening experiences a person can have — a sudden surge of intense fear that hits with pounding heart, shortness of breath, dizziness, and a genuine sense that something is catastrophically wrong, sometimes that you’re dying or losing your mind. Here’s a crucial thing to know: having a panic attack, even a severe one, does not mean you have panic disorder. Panic attacks are common. Panic disorder is something more specific — it’s when the attacks become recurrent and unexpected, and you begin living in fear of the next one, or changing your life to avoid it.
That distinction is the whole point of this panic disorder test. It screens not just for panic attacks, but for the pattern that defines panic disorder: the attacks themselves, plus the persistent anxiety about recurrence and the avoidance behaviors that can quietly take over daily life. It’s built on the DSM-5-TR diagnostic criteria (APA, 2022). 15 questions, private results. It’s a screening tool, not a diagnosis.
What Is Panic Disorder?
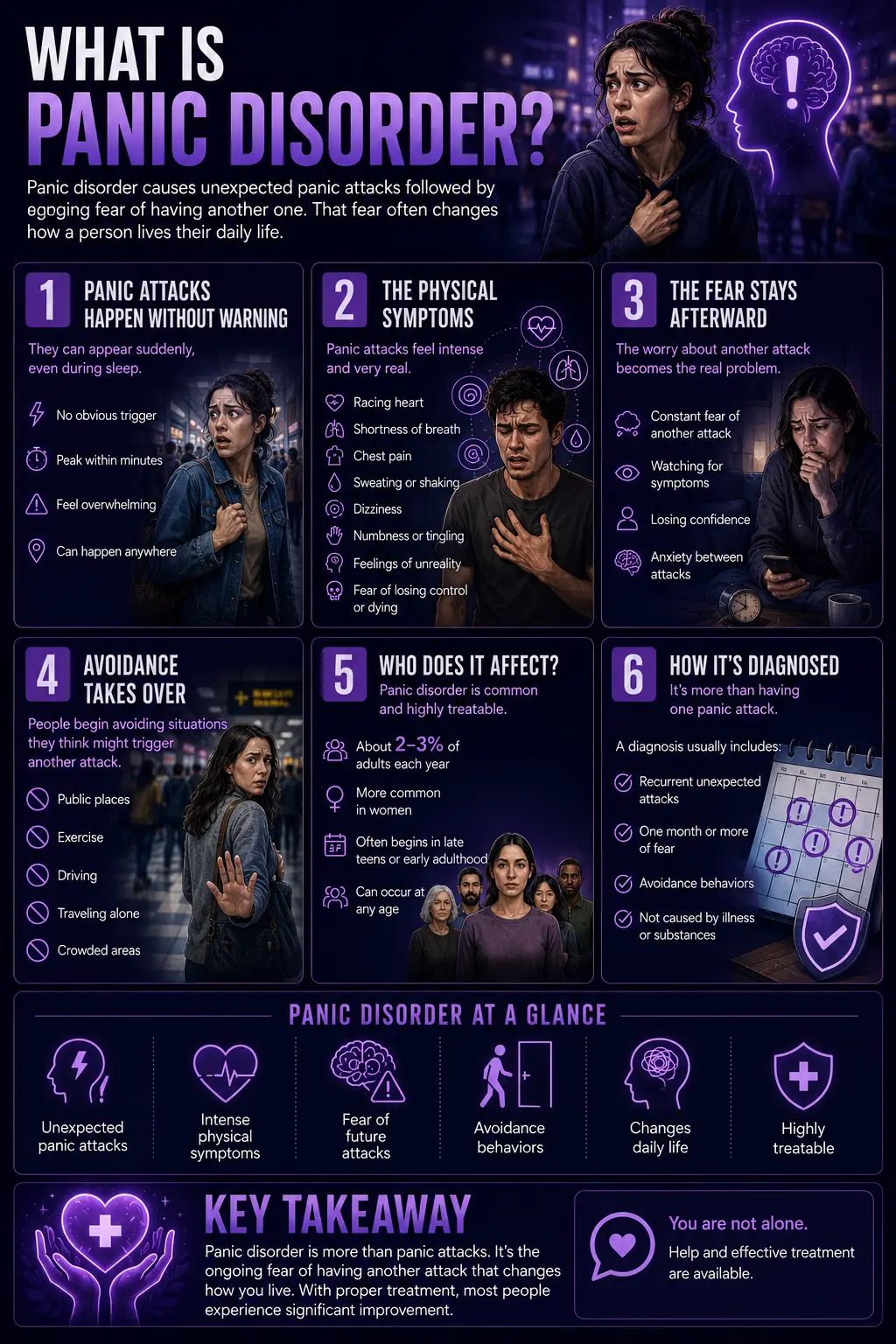
Panic disorder (DSM-5-TR code 300.01 / F41.0) is an anxiety disorder characterized by recurrent, unexpected panic attacks followed by at least a month of persistent worry about having more attacks, and/or significant changes in behavior aimed at avoiding them. It’s that second part — the ongoing fear and the behavior change — that separates panic disorder from simply experiencing panic attacks.
A panic attack is an abrupt surge of intense fear or discomfort that peaks within minutes, accompanied by at least four of thirteen recognized symptoms: pounding or racing heart, sweating, trembling or shaking, shortness of breath or a smothering feeling, a sense of choking, chest pain, nausea or stomach distress, dizziness or lightheadedness, chills or heat sensations, numbness or tingling, feelings of unreality or detachment, fear of losing control or “going crazy,” and fear of dying. The attacks in panic disorder are characteristically unexpected — they can come out of the blue, sometimes even waking a person from sleep, without an obvious trigger.
Panic disorder affects roughly 2–3% of people in a given year, with lifetime rates up to around 4.7%. It’s about twice as common in women as in men, and it typically begins in late adolescence or early adulthood, though it can start at any age. It commonly co-occurs with agoraphobia, generalized anxiety, and depression. Left untreated, it often follows a waxing-and-waning course — but it’s also one of the more treatable anxiety disorders, and treatment usually helps significantly.
The full DSM-5-TR criteria require: recurrent unexpected panic attacks (Criterion A); at least one month of persistent concern about additional attacks or their consequences, and/or a significant maladaptive change in behavior related to the attacks such as avoiding exercise or unfamiliar situations (Criterion B); the disturbance isn’t due to a substance or medical condition (Criterion C); and it isn’t better explained by another mental disorder (Criterion D). Notably, unlike generalized anxiety disorder, panic disorder has no six-month duration requirement — the one-month concern-or-behavior-change criterion is enough.
Panic Attack vs Panic Disorder — The Key Difference
This distinction matters enormously, because confusing the two causes needless worry for some people and missed diagnoses for others.
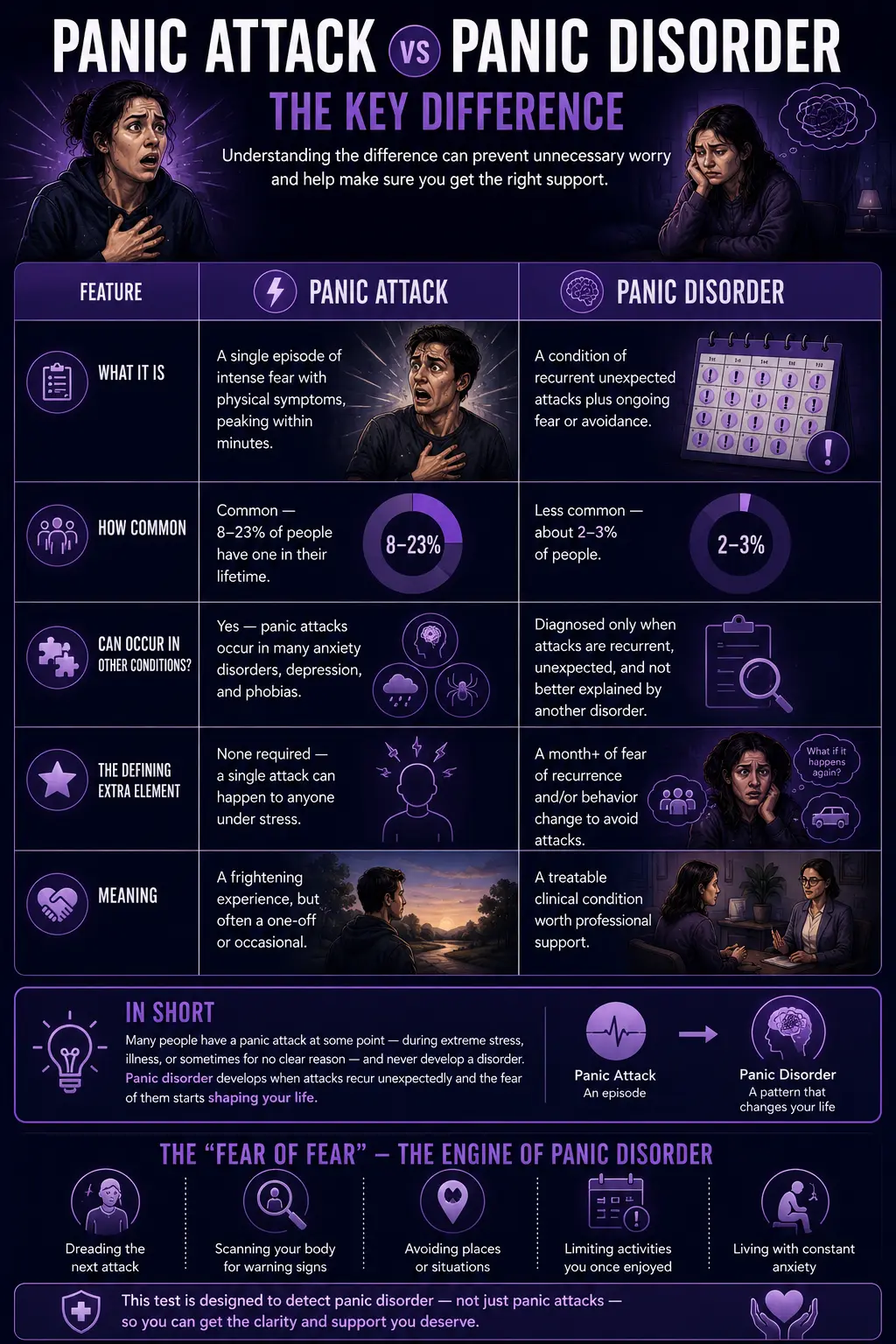
| Feature | Panic Attack | Panic Disorder |
|---|---|---|
| What it is | A single episode of intense fear with physical symptoms, peaking within minutes | A condition of recurrent unexpected attacks plus ongoing fear or avoidance |
| How common | Common — 8–23% of people have one in their lifetime | Less common — about 2–3% of people |
| Can occur in other conditions? | Yes — panic attacks occur in many anxiety disorders, depression, and phobias | Diagnosed only when attacks are recurrent, unexpected, and not better explained by another disorder |
| The defining extra element | None required — a single attack can happen to anyone under stress | A month+ of fear of recurrence and/or behavior change to avoid attacks |
| Meaning | A frightening experience, but often a one-off or occasional | A treatable clinical condition worth professional support |
In short: many people have a panic attack at some point — during extreme stress, illness, or sometimes for no clear reason — and never develop a disorder. Panic disorder is what can develop when the attacks recur unexpectedly, and the fear of them starts shaping your life. The “fear of fear” — dreading the next attack, scanning your body for warning signs, avoiding places or activities where an attack might happen — is the engine of panic disorder, and it’s what this test is designed to detect.
Signs You Might Have Panic Disorder
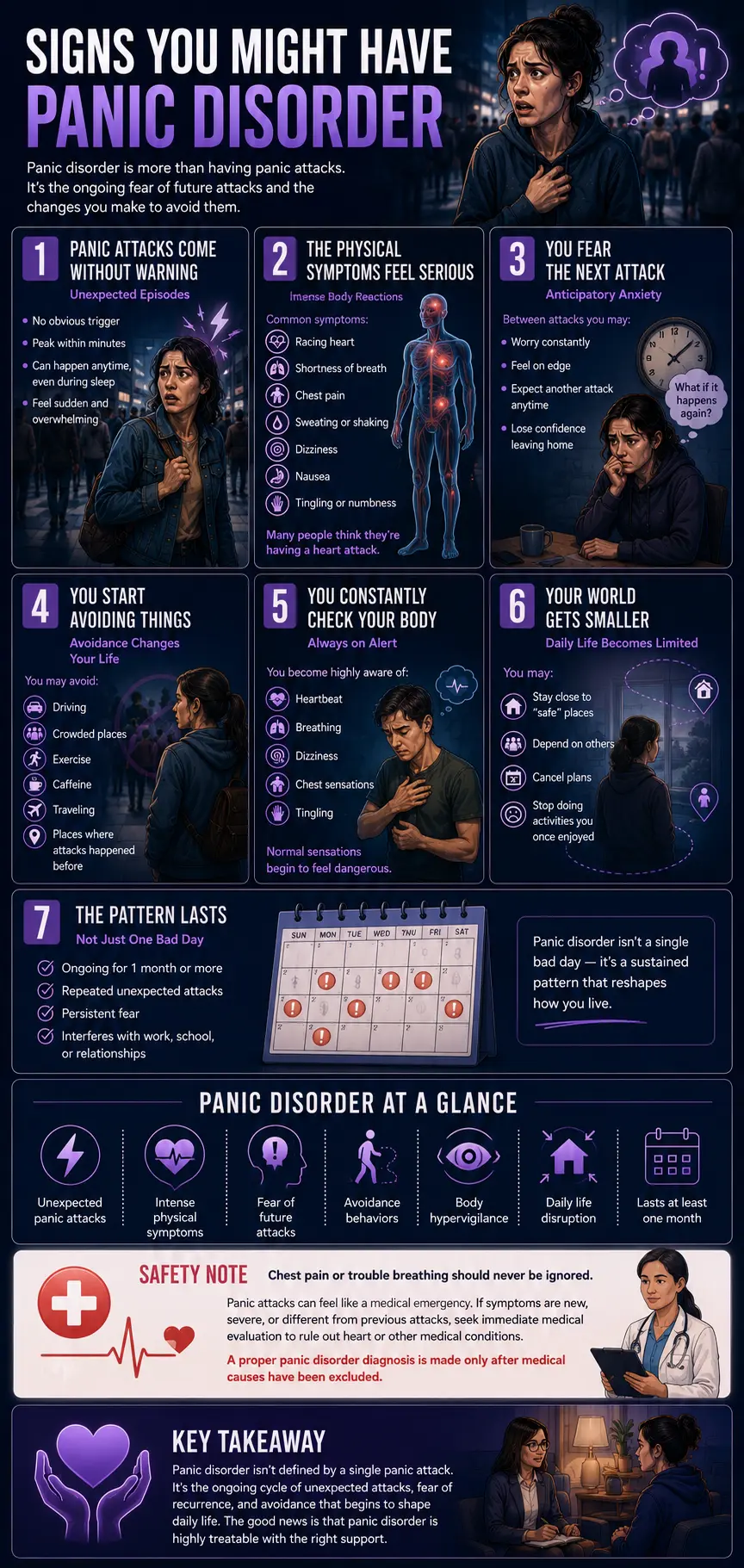
Panic disorder is more than the attacks themselves — it’s the whole pattern of recurrent attacks and the anxiety and avoidance that grow up around them. These are the signs most consistent with panic disorder, drawn from the DSM-5-TR criteria.
You have panic attacks that come out of the blue. Sudden surges of intense fear with physical symptoms — racing heart, breathlessness, dizziness, chest tightness — that arrive unexpectedly, without an obvious trigger. The unexpectedness is characteristic: panic disorder attacks aren’t always tied to a specific feared situation the way phobias are.
The physical symptoms are intense and frightening. Panic attacks hijack the body: pounding heart, shortness of breath, trembling, sweating, nausea, tingling, chills or heat. The symptoms are so physical that many people believe they’re having a heart attack or medical emergency — and end up in the ER, where tests come back normal.
You live in fear of the next attack. This is the core of panic disorder. Between attacks, you worry about when the next one will strike — a persistent, background dread often called “anticipatory anxiety.” The fear of the attack becomes its own ongoing problem, sometimes more disabling than the attacks themselves.
You fear what the attacks mean. Worry that the attacks signal something catastrophic — that you’ll lose control, “go crazy,” collapse, embarrass yourself, or that they indicate a serious undiagnosed illness. This fear of the consequences of attacks is part of the diagnostic picture.
You’ve started avoiding things because of the attacks. Changing your behavior to prevent attacks or to ensure you could escape or get help if one hit — avoiding exercise (because a racing heart feels like an attack), caffeine, crowded places, driving, being far from home, or situations where a previous attack occurred. This maladaptive behavior change is a defining feature.
You scan your body for warning signs. Hypervigilance to physical sensations — noticing every skipped heartbeat, wave of dizziness, or shortness of breath and interpreting it as the start of an attack. This body-monitoring can itself trigger attacks, creating a self-reinforcing cycle.
Your world is getting smaller. As avoidance grows, life narrows — fewer places you’ll go, fewer things you’ll do, more reliance on “safe” people or places. When avoidance expands to many situations where escape feels hard or help unavailable, it may signal agoraphobia, which frequently accompanies panic disorder.
The pattern has lasted, and it’s affecting your life. The fear or avoidance has persisted for at least a month and is interfering with work, relationships, or daily activities. Panic disorder isn’t a single bad day — it’s a sustained pattern that reshapes how you live.
A critical safety note: because panic attack symptoms — chest pain, shortness of breath, racing heart — overlap with genuine medical emergencies like heart problems, they should never simply be assumed to be “just anxiety.” Especially the first time, or if symptoms are new or different, these warrant medical evaluation to rule out cardiac and other conditions. A proper panic disorder diagnosis is made only after medical causes have been excluded.
How This Panic Disorder Test Works
This test contains 15 questions covering both parts of panic disorder: the panic attacks themselves and their symptoms, and — importantly — the anticipatory fear and avoidance behaviors that define the disorder. For each, choose how often it has applied to you recently: Never, Rarely, Sometimes, Often, or Always.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Your answers add up to a score from 0 to 60. Because panic disorder is defined by the fear-and-avoidance pattern lasting at least a month, answer with your recent experience in mind. This is a screening tool, not a diagnosis — and remember, a proper diagnosis also requires ruling out medical causes, which only a doctor can do.
Understanding Your Panic Disorder Test Score
| Score Range | Level | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Panic Indicators | Few signs of panic disorder. Occasional anxiety may be present without the recurrent-attack-and-fear pattern. |
| 16 – 30 | Mild — Some Panic Features | Some panic-related features present. Worth monitoring, and worth support if they’re causing distress. |
| 31 – 45 | Moderate — Significant Panic Features | A pattern consistent with panic disorder. A professional evaluation is recommended. |
| 46 – 60 | High — Strong Panic Indicators | Strong indicators of panic disorder, including fear and avoidance. A professional evaluation is strongly recommended. |
What Causes Panic Disorder?
Panic disorder arises from a combination of factors rather than a single cause. Genetics play a role — panic disorder runs in families, and having a first-degree relative with it raises risk. Neurobiologically, it involves the brain’s fear circuitry (particularly the amygdala and related structures) and systems regulating the body’s alarm response; people with panic disorder appear to have a more sensitive “fight or flight” system that can fire without real danger. Temperament matters too: a tendency toward anxiety, and “anxiety sensitivity” — the tendency to interpret normal physical sensations as dangerous — is a well-established risk factor.
Life stress often plays a role in onset, with the first attacks frequently emerging during a period of significant stress, loss, or transition. And once attacks begin, a powerful psychological cycle can take hold: an attack produces frightening sensations, the person becomes hypervigilant to those sensations and fears the next attack, that very hypervigilance and fear increase arousal, and the increased arousal makes further attacks more likely. This “fear of fear” cycle is what maintains panic disorder — and, helpfully, it’s exactly what effective treatment targets.
How Panic Disorder Is Treated
Panic disorder is highly treatable, and this is worth emphasizing because the condition itself makes people feel trapped. The two front-line treatments are psychotherapy and medication, used alone or together.
Cognitive Behavioral Therapy (CBT) is the gold-standard psychotherapy and is remarkably effective for panic disorder. It works by helping you understand what panic attacks actually are (not dangerous), reinterpret the physical sensations that feel catastrophic, and — through gradual, supported exposure — reduce the avoidance and the fear of the sensations themselves. Interoceptive exposure, which deliberately and safely brings on feared bodily sensations to reduce their power, is a particularly effective component. CBT directly breaks the fear-of-fear cycle.
Medication helps many people. SSRIs and SNRIs are commonly used first-line and can reduce the frequency and intensity of attacks. Other medications are sometimes used in specific situations under medical guidance. A healthcare provider can help weigh the options.
Self-management supports treatment: learning breathing and grounding techniques, reducing stimulants like caffeine, regular exercise (which, despite feeling counterintuitive when a racing heart is feared, helps over time), and stress management. But for panic disorder that’s affecting your life, professional treatment is the path that reliably works — self-help alone often isn’t enough to break an entrenched cycle, and there’s no reason to struggle without the effective help that exists.
Frequently Asked Questions
What is the difference between a panic attack and panic disorder?
A panic attack is a single episode of sudden, intense fear with physical symptoms (racing heart, shortness of breath, dizziness, chest pain) that peaks within minutes. Panic attacks are common — 8 to 23% of people have one in their lifetime — and can occur in many situations, including under stress or as part of other conditions. Panic disorder is a specific clinical condition: recurrent, unexpected panic attacks plus at least a month of persistent worry about having more attacks and/or significant changes in behavior to avoid them. In other words, having a panic attack doesn’t mean you have panic disorder — the disorder is defined by the attacks recurring unexpectedly and by the fear and avoidance that develop around them. Only about 2–3% of people have panic disorder.
Are panic attacks dangerous?
Panic attacks are intensely frightening but not physically dangerous in themselves — they’re the body’s fight-or-flight alarm system firing when there’s no actual threat. The sensations that feel catastrophic (racing heart, breathlessness, chest tightness, feeling you might die or lose control) are the alarm response, not signs of imminent harm, and they pass. That said, there’s an important caveat: because panic symptoms overlap with genuine medical emergencies like heart problems, panic should never simply be assumed — especially a first episode, or new or different symptoms, warrant medical evaluation to rule out physical causes. Once medical conditions are excluded and panic disorder is diagnosed, it’s genuinely reassuring to know the attacks, however awful, aren’t harming your body.
Can panic disorder be cured?
Panic disorder is one of the most treatable anxiety disorders, and many people achieve full, lasting relief. Cognitive Behavioral Therapy is highly effective — it directly targets the “fear of fear” cycle that maintains the disorder, helping people reinterpret the physical sensations and reduce avoidance, often with lasting results. Medication (commonly SSRIs or SNRIs) also helps many people, alone or combined with therapy. While “cure” is a strong word for any mental health condition, it’s fair to say that panic disorder responds very well to treatment, and a large proportion of people who get proper help see their attacks become infrequent or stop, and reclaim the parts of life that fear had narrowed.
Why do I have panic attacks for no reason?
The “unexpected,” out-of-the-blue quality is actually characteristic of panic disorder — unlike a phobia, where fear attaches to a specific trigger, panic disorder attacks often arrive without an obvious cause, sometimes even waking people from sleep. There usually is an underlying mechanism, though: a sensitized fear-response system, heightened sensitivity to bodily sensations (so a normal skipped heartbeat or wave of dizziness gets interpreted as danger and sets off the alarm), and often a background of stress. It can feel like the attacks come from nowhere, but they’re typically the body’s alarm system misfiring in response to internal sensations you may not consciously notice. Understanding this is part of why treatment helps — it makes the “random” attacks make sense and become manageable.
Is panic disorder the same as anxiety?
Not exactly — panic disorder is a specific type of anxiety disorder, but not all anxiety is panic disorder. Anxiety is a broad category. Generalized anxiety disorder, for instance, involves persistent, excessive worry about many things, building over time. Panic disorder is specifically about recurrent, sudden panic attacks and the fear and avoidance surrounding them — the fear is focused on the attacks themselves rather than diffuse life worries. They can overlap and co-occur, but they’re distinct. If your main experience is ongoing worry rather than discrete panic attacks, our GAD Test or general Anxiety Test may fit better.
What is the connection between panic disorder and agoraphobia?
They’re closely linked but, since the DSM-5, are diagnosed separately. Agoraphobia is fear or avoidance of situations where escape might be difficult or help unavailable if panic-like symptoms occurred — places like crowds, public transport, open spaces, or being far from home. It develops in roughly 30–50% of people with panic disorder, as avoidance of attack-associated situations gradually expands. Someone can have panic disorder without agoraphobia, agoraphobia without full panic disorder, or both together. If your avoidance has spread to many situations because of fear of panic, it’s worth exploring agoraphobia specifically with our Agoraphobia Test.
How is panic disorder diagnosed?
Panic disorder is diagnosed by a healthcare professional based on the DSM-5-TR criteria: recurrent unexpected panic attacks, followed by at least a month of persistent concern about more attacks and/or significant avoidance behavior, not better explained by another condition. An important first step is ruling out medical causes — conditions like thyroid problems, heart arrhythmias, asthma, and others can produce similar symptoms, so a medical evaluation is part of an accurate diagnosis. There’s no blood test or scan for panic disorder; diagnosis comes from a careful clinical assessment. This online test can help you recognize whether your experiences fit the pattern and decide whether to seek that evaluation, but it can’t diagnose the condition itself.
Related Tests
- Anxiety Test — a broader screen for general anxiety, useful if your experience is more diffuse worry than discrete panic attacks
- Agoraphobia Test — screens for fear and avoidance of situations where escape feels hard; develops in 30–50% of panic disorder cases
- Generalized Anxiety Disorder Test — for persistent, excessive worry across many areas of life, distinct from panic’s discrete attacks
- Social Anxiety Test — panic attacks triggered specifically by social situations may point here rather than to panic disorder
- Clinical Depression Test — depression commonly co-occurs with panic disorder and is worth screening alongside
- PTSD Test — panic attacks triggered by trauma reminders may relate to PTSD rather than panic disorder
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Panic Disorder 300.01 (F41.0), pp. 235–250. psychiatry.org
- Merck Manual / MSD Manual Professional Edition. (2026). Panic Attacks and Panic Disorder. [Prevalence 2-3%; panic attacks 8-23% lifetime; DSM-5-TR criteria; medical mimics] merckmanuals.com
- Asmundson, G.J., Taylor, S., & Smits, J.A. (2014). Panic disorder and agoraphobia: an overview and commentary on DSM-5 changes. Depression and Anxiety, 31(6), 480–486. [Separation of panic disorder and agoraphobia in DSM-5] onlinelibrary.wiley.com
- Kessler, R.C., Chiu, W.T., Jin, R., et al. (2006). The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication. Archives of General Psychiatry, 63(4), 415–424. [Lifetime prevalence data] pubmed.ncbi.nlm.nih.gov
- Locke, A.B., Kirst, N., & Shultz, C.G. (2015). Diagnosis and management of generalized anxiety disorder and panic disorder in adults. American Family Physician, 91(9), 617–624. [Diagnosis and treatment overview] aafp.org