
The fear that defines agoraphobia is not a fear of open spaces or crowds in themselves. It is the fear of what might happen there — specifically, the fear of being in a situation where escape would be difficult, where help would not be available, or where a panic attack, incapacitation, or humiliation might occur with no way out. The situation becomes threatening not because of what it contains but because of what it prevents: control, escape, rescue.
What begins as avoidance of a few uncomfortable situations can, without treatment, progressively expand until the safe zone becomes very small. More than one-third of people with agoraphobia become homebound and unable to maintain gainful employment, according to Analyze Psychiatry (2025). Untreated, the spontaneous remission rate is approximately 10% — agoraphobia does not typically resolve on its own (Analyze Psychiatry, 2025). These are not reasons for despair — they are reasons to take the pattern seriously and seek support before the world shrinks further.
This free Agoraphobia Test screens for agoraphobia using all five DSM-5-TR situational criteria and the full diagnostic framework (APA, 2022). 15 questions. Based on the past 6 months. Instant, private results.
What Is Agoraphobia?
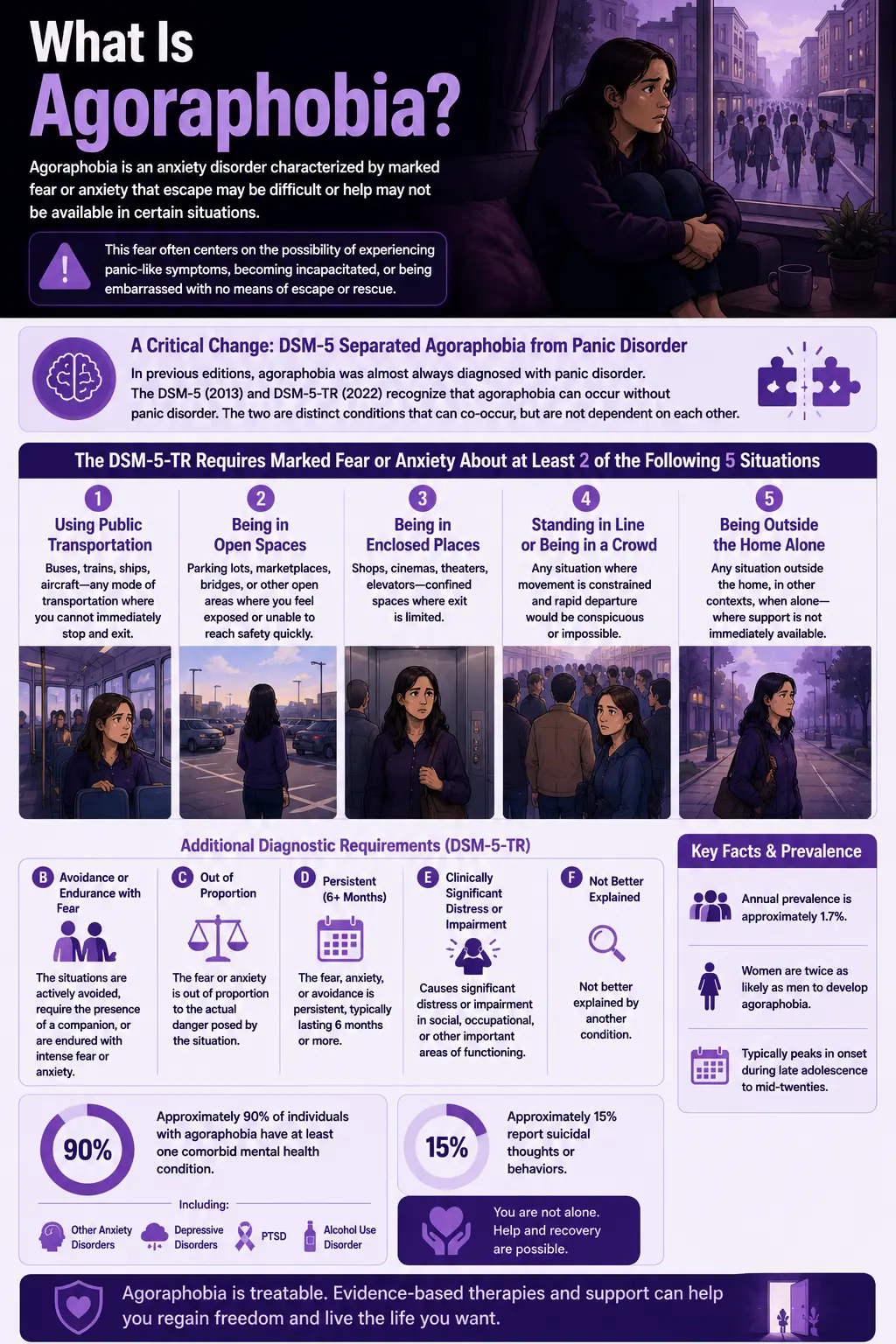
Agoraphobia is an anxiety disorder (DSM-5-TR code 300.22 / ICD-10: F40.00) characterized by marked fear or anxiety arising from thoughts that escape may be difficult or that help may not be available in certain situations. This fear often centers on the possibility of experiencing panic-like symptoms, becoming incapacitated, or being embarrassed with no means of escape or rescue (StatPearls, Balaram & Marwaha, 2024).
A critical change in how agoraphobia is understood came with the DSM-5 (2013): agoraphobia was formally separated from panic disorder. In previous editions, agoraphobia was almost always diagnosed in the context of panic disorder. The DSM-5 change — maintained in the DSM-5-TR (2022) — recognizes that a substantial number of individuals develop agoraphobia without experiencing panic disorder, and that the two are distinct conditions that can co-occur but are not dependent on each other (APA, DSM-5 Changes, 2013; StatPearls, 2024).
The DSM-5-TR requires marked fear or anxiety about at least 2 of the following 5 situations (APA, 2022):
- Situation 1 — Using public transportation: Buses, trains, ships, aircraft — any mode of transportation where you cannot immediately stop and exit.
- Situation 2 — Being in open spaces: Parking lots, marketplaces, bridges, or other open areas where you feel exposed or unable to reach safety quickly.
- Situation 3 — Being in enclosed places: Shops, cinemas, theaters, elevators — confined spaces where exit is limited.
- Situation 4 — Standing in line or being in a crowd: Any situation where movement is constrained and rapid departure would be conspicuous or impossible.
- Situation 5 — Being outside the home alone: Any situation outside the home, in other contexts, when alone — where support is not immediately available.
Additional diagnostic requirements (APA, 2022):
- Criterion B: The situations are actively avoided, require the presence of a companion, or are endured with intense fear or anxiety.
- Criterion C: The fear or anxiety is out of proportion to the actual danger posed by the situation.
- Criterion D: The fear, anxiety, or avoidance is persistent, typically lasting 6 months or more.
- Criterion E: The fear, anxiety, or avoidance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- Criterion F: Not better explained by another condition.
Annual prevalence is approximately 1.7% (Analyze Psychiatry, 2025). Women are twice as likely as men to develop agoraphobia (Analyze Psychiatry, 2025). The disorder typically peaks in onset during late adolescence to mid-twenties (Analyze Psychiatry, 2025; Psychiatry Investigation). Approximately 90% of individuals with agoraphobia have at least one comorbid mental health condition — including other anxiety disorders, depressive disorders, PTSD, or alcohol use disorder (StatPearls, Balaram & Marwaha, 2024 — DSM-5-TR figure). Approximately 15% report suicidal thoughts or behaviors (StatPearls, Balaram & Marwaha, 2024).
Signs You Might Have Agoraphobia
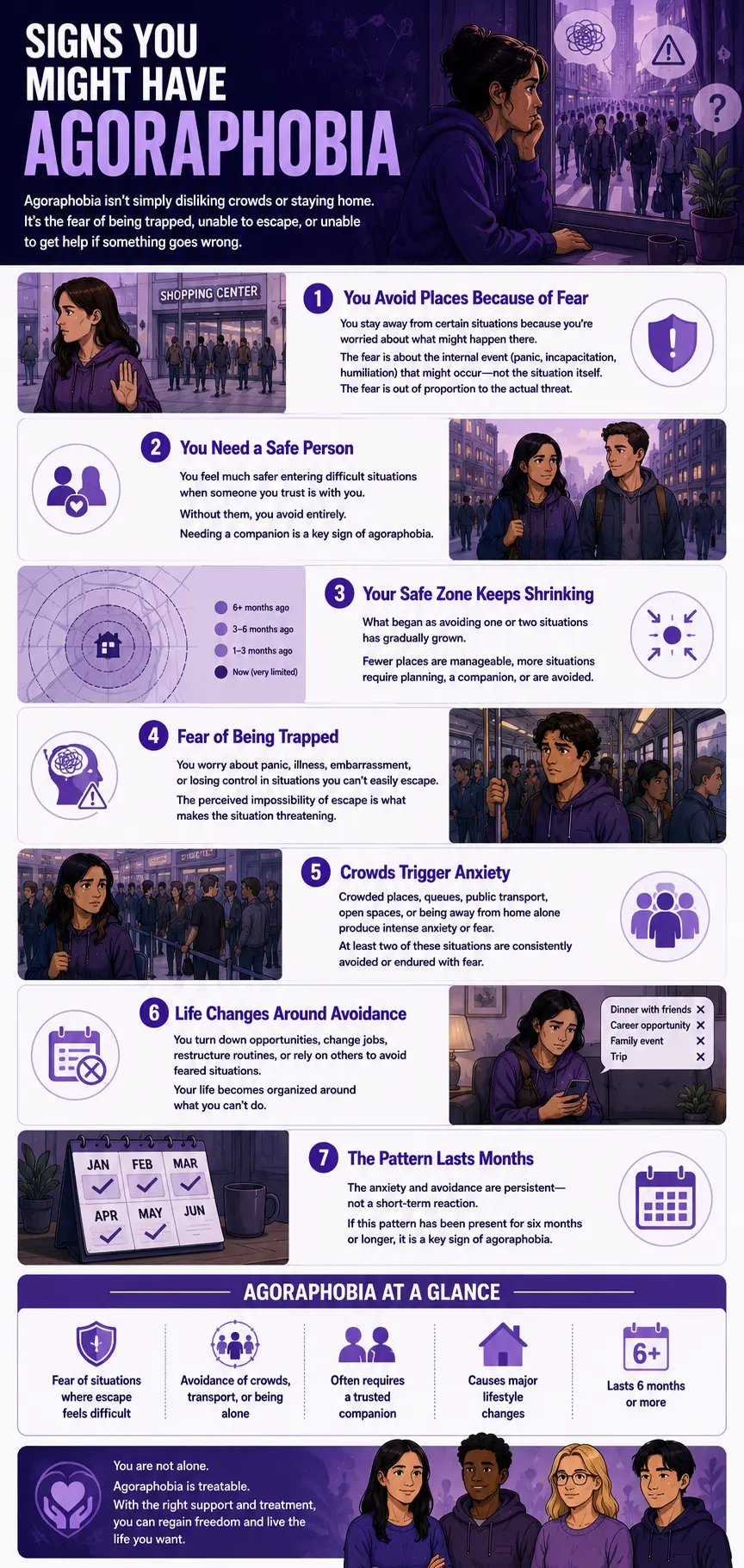
Agoraphobia is frequently misunderstood — and therefore frequently unrecognized. People may attribute their avoidance to introversion, preference, or reasonable caution, without recognizing that the avoidance has been progressively expanding and is driven by fear rather than choice. These are the signs that most consistently indicate agoraphobia may be present:
You avoid specific situations not because you dislike them but because you fear what might happen there. The avoidance is not preference — it is protective. You may recognize that the situation itself is not objectively dangerous. The fear is about the internal event (panic, incapacitation, humiliation) that might occur there, not about the external situation. This disproportionality — fear out of proportion to the actual threat — is DSM-5-TR Criterion C, and it is the core feature that distinguishes agoraphobia from reasonable caution.
You require a companion to enter situations you would otherwise avoid. The presence of a trusted person makes the feared situations manageable or tolerable. Without them, you avoid entirely. DSM-5-TR Criterion B explicitly recognizes the companion requirement as a diagnostic feature of agoraphobia — the need for a specific person to be present as a safety mechanism is not just anxiety but agoraphobia-specific avoidance.
The avoidance has been expanding over time. What began as avoiding one or two situations has gradually grown. The safe zone has been shrinking — fewer places are manageable, more situations require planning or a companion, or are avoided altogether. This progressive narrowing is one of the most reliable markers that the pattern is agoraphobia rather than ordinary anxiety.
You are afraid of having a panic attack, becoming incapacitated, or being embarrassed in situations you can’t easily escape. The feared outcome is not the situation but what might happen to you within it — a panic attack, a medical emergency, losing control, or some other incapacitating experience — with no exit available. The perceived impossibility of escape is what makes the situation threatening, not the situation itself.
Crowded places, queues, public transport, or being away from home alone produce intense anxiety or fear. At least two of the five DSM-5-TR agoraphobic situations are consistently avoided or endured with fear. The anxiety is not mild social discomfort — it is marked fear that the person recognizes as disproportionate but cannot fully control.
You have made significant changes to your daily life to accommodate the avoidance. Changed jobs, turned down social or professional opportunities, restructured your daily routine, or become increasingly dependent on specific people — to avoid the feared situations. The functional impact of the avoidance (DSM-5-TR Criterion E) is one of the most important markers of clinical significance. How much of your life has been reorganized around what you cannot do?
The anxiety or avoidance has been present for at least six months. DSM-5-TR Criterion D requires that the pattern is persistent — not a recent reaction to a stressful period that will resolve with time. If avoidance has been present for six months or longer across different contexts and moods, its chronicity is diagnostically significant.
Agoraphobia vs Panic Disorder vs Social Anxiety — The Critical Distinctions
These three conditions are frequently confused because they share anxiety symptoms and avoidance behaviors. The distinctions are clinically important because they affect the treatment approach.
| Feature | Agoraphobia | Panic Disorder | Social Anxiety Disorder |
|---|---|---|---|
| Core fear | Being in situations where escape is difficult or help is unavailable — fear of being trapped without exit or rescue | Having unexpected panic attacks and their consequences — fear of the attack itself, not primarily of the situation | Being negatively evaluated, humiliated, or embarrassed by others — fear of social judgment specifically |
| Avoided situations | 5 specific DSM-5-TR situational clusters: public transport, open spaces, enclosed spaces, crowds, being outside alone | May develop agoraphobia as a comorbidity; avoidance driven by anticipated panic rather than entrapment fear | Social situations where scrutiny or evaluation by others may occur — not primarily about escape or entrapment |
| Role of companion | A trusted companion enables entry into feared situations — companion = safety signal for escape/rescue | May use companions, but the core fear is the panic attack, not entrapment | Companions do not typically enable entry into feared situations — social evaluation is the feared outcome regardless |
| DSM-5-TR relationship | Separate diagnosis since DSM-5 (2013) — can co-occur with panic disorder but is independent | No longer requires agoraphobia to be present — diagnosed independently; can co-occur with agoraphobia | Distinct anxiety disorder — may co-occur with agoraphobia but is a separate diagnosis |
| Duration criterion | 6 months+ (all ages, per DSM-5-TR) | 1 month+ of persistent concern or behavior change following attacks | 6 months+ (all ages, per DSM-5-TR) |
| PsyMed test | This test | Anxiety Test | Social Anxiety Test |
An important clinical note: agoraphobia and panic disorder co-occur frequently — before the DSM-5 separated them, they were diagnosed together by default. The separation in DSM-5 and DSM-5-TR recognizes that many people with agoraphobia do not have panic disorder, and many people with panic disorder do not develop agoraphobia. When both are present, both diagnoses are recorded, and both are treatment targets (APA, DSM-5 Changes, 2013).
What Causes Agoraphobia?
The role of panic attacks and panic disorder. While agoraphobia can develop without panic disorder, panic attacks are a common precipitant. The experience of an unexpected panic attack in a specific situation can trigger the learning process that underpins agoraphobia: if a panic attack occurred in a supermarket, the supermarket becomes associated with danger; avoidance of the supermarket reduces the anxiety, which reinforces the avoidance behavior. This conditioning process gradually extends to other situations associated with the feared outcome (StatPearls, Balaram & Marwaha, 2024).
Behavioral conditioning and avoidance reinforcement. Avoidance is the central maintenance mechanism of agoraphobia. Each time the feared situation is avoided and the anxiety is reduced, the avoidance behavior is reinforced — making it more likely to recur and extend to adjacent situations. Over time, the safe zone contracts because the conditioning process extends to situations that share features with the originally feared ones (StatPearls, Balaram & Marwaha, 2024).
Cognitive factors. Catastrophic misinterpretation of physical sensations — interpreting a racing heartbeat as a sign of a heart attack, dizziness as a sign of fainting, or breathlessness as a sign of suffocation — amplifies anxiety in ways that make the feared situations feel genuinely dangerous. The cognitive model of agoraphobia proposes that the disorder is maintained by this misinterpretation cycle: sensation → catastrophic interpretation → anxiety escalation → avoidance (Analyze Psychiatry, 2025).
Neurobiological factors. Abnormalities in the fear circuitry — particularly in the amygdala, which mediates threat detection and fear responses — are documented in anxiety disorders including agoraphobia. Dysregulation in serotonergic and noradrenergic neurotransmitter systems contributes to the heightened baseline anxiety that makes agoraphobic responses more likely.
Comorbidities. As noted, approximately 90% of people with agoraphobia have at least one comorbid condition (StatPearls, Balaram & Marwaha, 2024). The most common are other anxiety disorders (including generalized anxiety, social anxiety, and specific phobias), major depressive disorder, PTSD, and alcohol use disorder. Approximately 15% of people with agoraphobia report suicidal thoughts or behaviors — making assessment of suicidality important when agoraphobia is identified (StatPearls, Balaram & Marwaha, 2024).
How This Test Works
This Agoraphobia Test covers all five DSM-5-TR situational criteria (APA, 2022) and the key clinical dimensions of agoraphobia — fear and avoidance in each situation cluster, the companion requirement, the disproportionality of fear, functional impairment, and the chronicity of the pattern — across 15 questions.
Answer based on your consistent experience over the past 6 months — the duration specified in DSM-5-TR Criterion D. Not your best or worst days, but the recurring pattern.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. This is a screening tool — only a qualified mental health professional can diagnose agoraphobia through comprehensive clinical assessment.
Understanding Your Agoraphobia Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Agoraphobia Indicators | Responses suggest few significant agoraphobia patterns. Occasional discomfort in crowded or confined spaces may be present without a pattern consistent with agoraphobic disorder. |
| 16 – 30 | Mild — Some Agoraphobic Patterns Present | Some agoraphobic patterns present — avoidance or significant anxiety in at least some of the five situational clusters. Warrants attention and professional discussion. |
| 31 – 45 | Moderate — Significant Agoraphobia Pattern | Significant agoraphobia pattern across multiple situational clusters, consistent with clinical agoraphobia. Professional evaluation and treatment are recommended. |
| 46 – 60 | High — Strong Agoraphobia Indicators | Severe agoraphobia pattern across most situations. Professional evaluation and treatment are strongly recommended. The world has likely been significantly restricted by the avoidance. |
Treatment for Agoraphobia
Agoraphobia is highly treatable. According to the Merck Manual (2026) and StatPearls (Balaram & Marwaha, 2024), effective treatments include:
Cognitive Behavioral Therapy (CBT) with Graduated Exposure. The most evidence-supported psychological treatment for agoraphobia. CBT targets the cognitive distortions that maintain the fear (catastrophic misinterpretation of physical sensations, overestimation of danger) and the avoidance behaviors that maintain the disorder through systematic, graduated exposure — beginning with the least feared situations and progressively working toward the most feared. The exposure component is essential: anxiety reduction through avoidance maintains agoraphobia; anxiety reduction through confrontation eliminates it.
Interoceptive Exposure. A specific component of CBT for agoraphobia involves deliberate induction of the feared physical sensations (dizziness, racing heart, breathlessness) in a safe context — decoupling the sensations from the catastrophic interpretations. Particularly important when panic symptoms are prominent (StatPearls, Balaram & Marwaha, 2024).
Pharmacotherapy — SSRIs and SNRIs. First-line medications for agoraphobia. Selective serotonin reuptake inhibitors (sertraline, paroxetine, escitalopram) and serotonin-norepinephrine reuptake inhibitors (venlafaxine) significantly reduce baseline anxiety and panic frequency, making the exposure work in CBT more accessible. Benzodiazepines may provide short-term relief but are not recommended long-term due to dependence risk and potential interference with the extinction learning that CBT produces.
Combination treatment. CBT combined with pharmacotherapy produces the strongest outcomes for moderate-to-severe agoraphobia. The medication reduces the baseline anxiety intensity enough to make the graduated exposure manageable; the exposure produces the lasting cognitive and behavioral change that medication alone does not (Merck Manual, 2026).
Frequently Asked Questions
What is agoraphobia?
Agoraphobia is an anxiety disorder (DSM-5-TR 300.22 / F40.00) characterized by marked fear or anxiety about at least 2 of 5 specific situational clusters — public transportation, open spaces, enclosed spaces, crowds, or being outside the home alone — where escape might be difficult or help might not be available. The situations are actively avoided, require a companion, or are endured with intense fear. The fear is out of proportion to actual danger, persistent for 6+ months, and causes clinically significant distress or functional impairment. Annual prevalence is approximately 1.7%, with women twice as likely as men to develop the disorder. About 90% of individuals have at least one comorbid condition (StatPearls, Balaram & Marwaha, 2024).
Is agoraphobia just a fear of open spaces?
No — this is one of the most common misconceptions about agoraphobia. The term derives from the Greek “agora” (marketplace) and has historically been associated with open spaces, but the DSM-5-TR definition is much broader and more precise. Agoraphobia is fundamentally about situations where escape might be difficult, or help might not be available — including enclosed spaces (cinemas, elevators), crowds and queues, public transport, and being outside alone. Many people with agoraphobia are actually more distressed in enclosed spaces than in open ones. The unifying feature is the perceived impossibility of escape or rescue, not the openness of the space.
What is the difference between agoraphobia and panic disorder?
Agoraphobia and panic disorder are now separate diagnoses in the DSM-5-TR (2022), having been separated in the DSM-5 (2013). Panic disorder involves recurrent unexpected panic attacks with persistent concern about future attacks and behavioral changes driven by that concern. Agoraphobia involves marked fear and avoidance of the five situational clusters where escape is perceived as difficult — regardless of whether panic attacks are present. A substantial number of people with agoraphobia do not have panic disorder (APA, 2013). When both are present, both diagnoses are recorded. The two conditions share treatment approaches (CBT, SSRIs) but each has specific components — interoceptive exposure is particularly important when panic disorder is also present.
Can agoraphobia develop without panic attacks?
Yes — and this is precisely why the DSM-5 separated them in 2013. Research documented that a significant proportion of people develop agoraphobia in response to feared experiences other than panic attacks — including fear of falling (particularly in older adults), fear of incontinence, fear of cardiac symptoms, or other embarrassing or incapacitating events. The separation recognizes that the core fear in agoraphobia is about being in a situation where escape is difficult or help is unavailable, not specifically about panic attacks (APA, DSM-5 Changes, 2013; StatPearls, Balaram & Marwaha, 2024).
Can agoraphobia be treated?
Yes — agoraphobia is highly treatable. Cognitive Behavioral Therapy with graduated exposure is the most evidence-supported psychological treatment, and SSRIs/SNRIs are the first-line pharmacological option. Combination treatment produces the strongest outcomes for moderate-to-severe presentations. The critical clinical reality is that agoraphobia does not typically resolve on its own — the spontaneous remission rate without treatment is approximately 10% (Analyze Psychiatry, 2025). The avoidance that provides short-term relief is the same mechanism that maintains and worsens the disorder long-term. Treatment works by systematically reversing the avoidance through supported, graduated exposure.
How does agoraphobia affect daily life?
Agoraphobia affects daily life primarily through the progressive restriction of functional independence. In mild cases, specific situations are avoided with minimal overall impact. In moderate cases, work, social activities, and relationships are significantly affected. In severe cases, more than one-third of individuals with agoraphobia become homebound and unable to maintain gainful employment (Analyze Psychiatry, 2025). The disorder affects relationships because dependence on companions for basic activities creates strain; it affects employment because workplaces, commutes, and professional environments may all fall within the feared situational clusters; and it affects quality of life because the anticipatory anxiety about potential exposures produces a continuous background dread that persists even when the feared situations are being successfully avoided.
What is the difference between agoraphobia and scopophobia?
Scopophobia is the intense fear of being watched, observed, or stared at by others — a specific phobia focused on the experience of being the object of others’ gaze. Agoraphobia is the fear of being in situations where escape is difficult or help is unavailable. While both conditions may produce avoidance of public spaces, the underlying fear is different: the scopophobic person avoids public spaces because they may be observed; the agoraphobic person avoids them because escape might be difficult. If the primary fear is being watched or stared at rather than being trapped, the Scopophobia Test may be a more precise fit. Both conditions can co-occur.
Related Tests
- Anxiety Test — generalized anxiety is the most common agoraphobia comorbidity; approximately 90% of people with agoraphobia have at least one comorbid condition
- Social Anxiety Test — social anxiety disorder and agoraphobia share avoidance of public situations but through different fear mechanisms; important to distinguish
- Scopophobia Test — fear of being watched or stared at; frequently confused with agoraphobia as both produce avoidance of public spaces
- PTSD Test — PTSD is a documented agoraphobia comorbidity; avoidance patterns in PTSD can overlap with agoraphobic avoidance
- Clinical Depression Test — depression is among the most common comorbidities of agoraphobia, particularly in severe cases where the disorder has significantly restricted functioning
- Burnout Test — chronic anxiety and avoidance produce a specific exhaustion; burnout and anxiety disorders frequently co-occur
- OCD Test — OCD avoidance can resemble agoraphobic avoidance; important to assess whether avoidance is driven by obsessional content or agoraphobic fear
- Dissociation Test — dissociative symptoms can occur during panic attacks and in agoraphobic situations; worth assessing where derealization or depersonalization are present during feared situations
- Avoidant Personality Disorder Test — AVPD involves pervasive social avoidance driven by inadequacy fears; agoraphobia involves situational avoidance driven by entrapment fears; both can co-occur
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Agoraphobia 300.22 (F40.00). psychiatry.org
- American Psychiatric Association. (2013). Highlights of Changes from DSM-IV-TR to DSM-5: Separation of agoraphobia from panic disorder. psychiatry.org
- Balaram, K., & Marwaha, R. (2024). Agoraphobia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. NBK554387. Updated November 11, 2024. [90% comorbidity; 15% suicidal ideation] ncbi.nlm.nih.gov
- Analyze Psychiatry. (2025). Agoraphobia — Signs, DSM-5 Criteria and Treatments. [1.7% annual prevalence; women 2x; >33% homebound; 10% remission untreated] analyzepsych.com
- Merck Manual Professional Edition. (2026). Agoraphobia. merckmanuals.com
- Psychiatry Investigation. (2024). The Burden of Agoraphobia in Worsening Quality of Life. [1 in 70 lifetime; female OR=2.23] psychiatryinvestigation.org
- Theravive. (2025). Agoraphobia DSM-5 300.22 (F40.00). theravive.com
- Wikipedia. (2025). Agoraphobia. en.wikipedia.org