
Most people have eaten past the point of comfort — at a celebration, during a stressful period, in the quiet of a difficult evening. That is not what Binge Eating Disorder describes. What BED describes is something more specific and more consuming: recurrent episodes of eating an objectively large amount of food in a discrete period of time, accompanied by a felt loss of control — the sense that you cannot stop, cannot regulate what or how much you are eating — and followed by significant distress: guilt, shame, disgust, or depression that persists long after the episode ends.
Binge Eating Disorder is the most common eating disorder in the United States and Western Europe — more prevalent than anorexia nervosa and bulimia nervosa combined (Hudson et al., Biological Psychiatry, 2007). It affects men and women across the weight spectrum, across age groups, and across ethnicities. And it is significantly underdiagnosed: only 43.6% of people with BED ever seek treatment specifically for the disorder, according to the National Comorbidity Survey Replication (NIMH, NCS-R).
This free Binge Eating Disorder Test screens for BED using the full DSM-5-TR diagnostic framework (APA, 2022), covering all five behavioral criteria and the complete diagnostic picture. 15 questions. Based on the past 3 months. Instant, private results.
If you are struggling with an eating disorder and need support, the National Alliance for Eating Disorders helpline is available at 1-866-662-1235 (Monday–Friday, 9am–5pm ET). For after-hours crisis support, contact the Crisis Text Line by texting NEDA to 741741.
What Is Binge Eating Disorder?
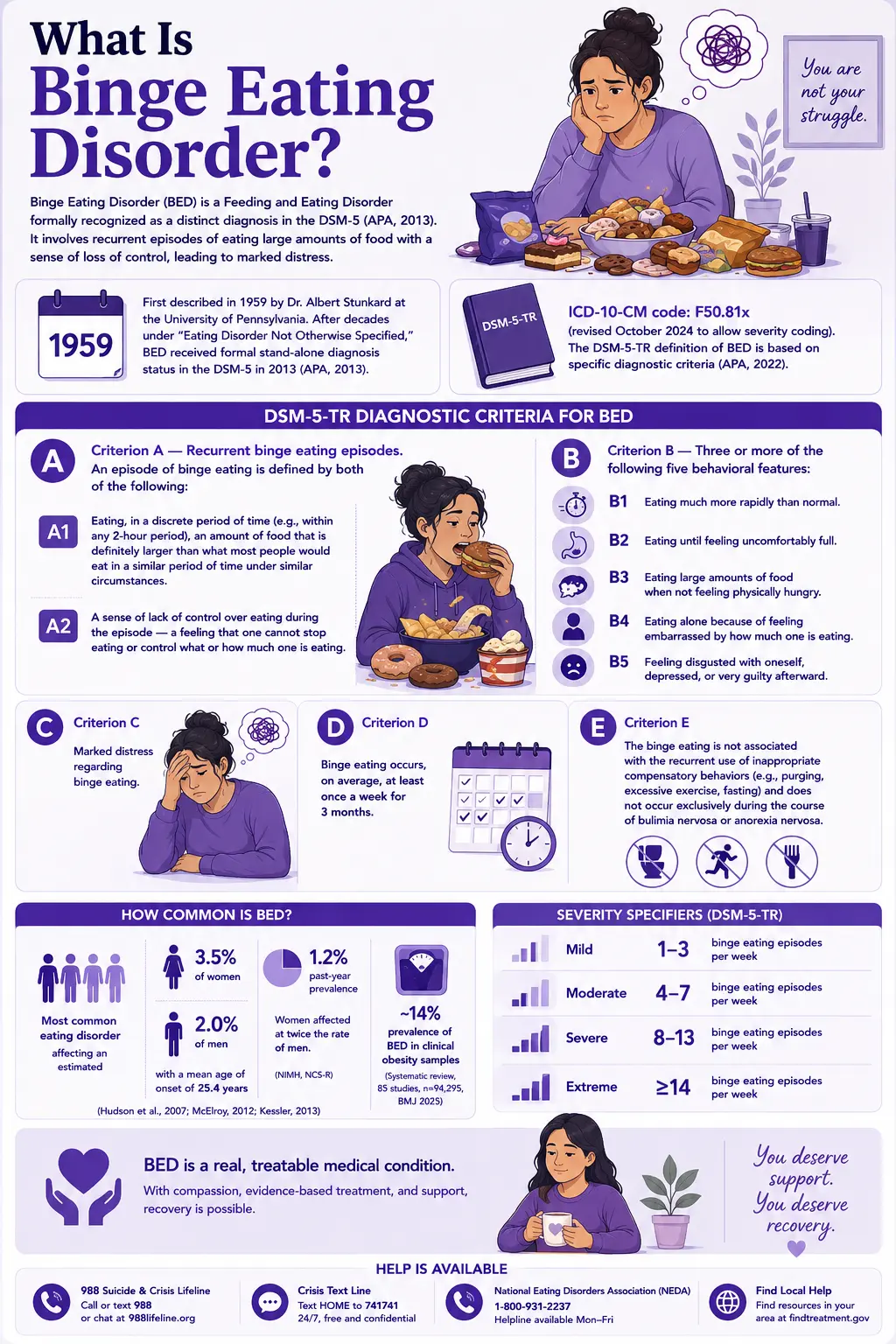
Binge Eating Disorder (BED) is a Feeding and Eating Disorder formally recognized as a distinct diagnosis in the DSM-5 (APA, 2013). Its ICD-10-CM code is F50.81x (revised October 2024 to allow severity coding). BED was first described in 1959 by Dr. Albert Stunkard at the University of Pennsylvania, who recognized recurrent episodes of uncontrolled overeating as a distinct clinical phenomenon. After decades of classification under “Eating Disorder Not Otherwise Specified,” BED received formal stand-alone diagnosis status in the DSM-5 in 2013 (APA, 2013), reflecting accumulated evidence of its distinct clinical profile, neurobiological basis, and treatment response.
The DSM-5-TR definition of BED requires (APA, 2022):
Criterion A — Recurrent binge eating episodes. An episode of binge eating is defined by both of the following:
- A1. Eating, in a discrete period of time (e.g., within any 2-hour period), an amount of food that is definitely larger than what most people would eat in a similar period of time under similar circumstances.
- A2. A sense of lack of control over eating during the episode — a feeling that one cannot stop eating or control what or how much one is eating.
Criterion B — Three or more of the following five behavioral features:
- B1. Eating much more rapidly than normal.
- B2. Eating until feeling uncomfortably full.
- B3. Eating large amounts of food when not feeling physically hungry.
- B4. Eating alone because of feeling embarrassed by how much one is eating.
- B5. Feeling disgusted with oneself, depressed, or very guilty afterward.
Criterion C. Marked distress regarding binge eating.
Criterion D. Binge eating occurs, on average, at least once a week for 3 months.
Criterion E. The binge eating is not associated with the recurrent use of inappropriate compensatory behaviors (e.g., purging, excessive exercise, fasting) and does not occur exclusively during the course of bulimia nervosa or anorexia nervosa.
BED is the most common eating disorder, affecting an estimated 2.5% of adults — approximately 3.5% of women and 2.0% of men — with a mean age of onset of approximately 25.4 years (Hudson et al., 2007; McElroy, 2012; Kessler, 2013). Past-year prevalence is 1.2%, with women affected at twice the rate of men (NIMH, NCS-R). The disorder is significantly more prevalent among people seeking obesity treatment, with BED prevalence of approximately 14% in clinical obesity samples (systematic review, 85 studies, n=94,295, BMJ 2025).
Severity specifiers (DSM-5-TR):
- Mild: 1–3 binge eating episodes per week
- Moderate: 4–7 episodes per week
- Severe: 8–13 episodes per week
- Extreme: ≥14 episodes per week.
Signs You Might Have Binge Eating Disorder
BED is one of the most consistently underrecognized eating disorders — partly because it does not involve the compensatory behaviors (purging, restriction) that most people associate with eating disorders, partly because it occurs across all body sizes and therefore doesn’t “look like” what people imagine, and partly because the shame embedded in the disorder itself makes disclosure extraordinarily difficult. These are the patterns that most consistently indicate BED may be present:
You eat an amount of food that you know is objectively large — and you feel unable to stop. This is not eating more than intended because the food was delicious. It is a distinct experience of loss of control — the sense that stopping is not fully available to you once the episode has begun, that something has shifted and the eating continues past the point of choice. The quantity involved is objectively large — more than most people would eat in that same period under similar circumstances. This is DSM-5-TR Criterion A: both the quantity and the loss of control must be present.
You eat much faster than usual during these episodes. A characteristic behavioral feature of binge eating (DSM-5-TR Criterion B1) is the speed of eating — consuming food rapidly, without the ordinary pace of a meal. The speed reflects the loss of regulation that defines the episode: the normal pacing signals that moderate eating have been overridden.
You continue eating until you are uncomfortably — sometimes painfully — full. DSM-5-TR Criterion B2: eating past the point of comfortable satiation, continuing to the point of physical discomfort or pain. Eating continues despite these internal signals because the regulatory system that typically responds to fullness is not functioning as usual during the episode.
You eat large amounts when you are not physically hungry. DSM-5-TR Criterion B3 specifically captures eating that is disconnected from physical hunger — driven by emotional state, habit, distress, or compulsion rather than the body’s need for food. Binge eating frequently serves as a regulatory response to negative emotional states: anxiety, loneliness, boredom, distress, or a dysphoric mood that eating temporarily alleviates.
You eat alone because of embarrassment about the amount. DSM-5-TR Criterion B4: eating in secret, hiding the eating from others, arranging situations so that the eating can happen without observation. The concealment itself is a significant clinical signal — it reflects the shame embedded in the episode and produces the social isolation that both accompanies and amplifies BED over time.
After the episode, you feel disgusted with yourself, deeply depressed, or intensely guilty. DSM-5-TR Criterion B5: significant negative emotions directed at the self in the aftermath of the episode. This is typically not mild regret — it is intense self-disgust, shame, guilt, or depression that can persist for hours after the episode ends. These post-episode emotions frequently trigger subsequent episodes as the person attempts to regulate those painful feelings through eating, creating a cycle that is self-reinforcing.
The episodes occur regularly — and have been occurring for at least 3 months. A single episode or occasional episodes during exceptional stress are not BED. The DSM-5-TR requires at least once weekly for 3 months (Criterion D). If the pattern has been consistent and recurring across different emotional states, different circumstances, and different periods, that recurrence is itself diagnostically significant.
The eating feels out of your control in a way that other eating does not. This is the core distinguishing feature. People with BED frequently describe two modes of eating — normal eating and binge eating — that feel qualitatively different from each other. The binge eating feels driven, compelled, or autonomous in a way that ordinary eating does not. The felt loss of control is not metaphorical; it reflects actual dysregulation in the reward, impulse-control, and emotion-regulation systems that govern eating behavior.

BED vs Bulimia Nervosa vs Emotional Eating vs Overeating — The Critical Distinctions
| Feature | Occasional Overeating | Emotional Eating | Binge Eating Disorder (BED) | Bulimia Nervosa (BN) |
|---|---|---|---|---|
| Amount of food | More than intended; proportionate to appetite/enjoyment | Variable, driven by emotional state, not always objectively large | Objectively large amount — more than most people would eat in the same period (DSM Criterion A1) | Objectively large amount — same as BED definition |
| Loss of control | Not present — could stop if motivated | May be present but not always; variable | Core feature — felt inability to stop or regulate (DSM Criterion A2) | Core feature — same as BED |
| Compensatory behaviors | None | None typically | None — absence of compensatory behavior is a diagnostic requirement (DSM Criterion E) | Present and recurrent — purging, fasting, excessive exercise (required for diagnosis) |
| Post-episode distress | Mild discomfort; proportionate regret | Variable; some guilt, typically not severe or persistent | Marked distress — shame, guilt, self-disgust, depression (DSM Criterion C) | Significant distress drives the compensatory behavior |
| Frequency | Infrequent; no pattern | Variable; tied to emotional states | At least once weekly for 3+ months (DSM Criterion D) | At least once weekly for 3+ months (same criterion) |
| DSM-5-TR classification | Not a disorder | Not a standalone diagnosis | Feeding and Eating Disorder (F50.81x) | Feeding and Eating Disorder (F50.2) |
| PsyMed assessment | No screening needed | Consider Anxiety Test or Depression Test | This test | Eating Disorder Test |
What Causes Binge Eating Disorder?
BED develops from an interaction of neurobiological, psychological, and environmental factors. According to Medscape (2025), BED frequently develops in the context of underlying vulnerabilities, including disturbances in reward processing, impaired inhibitory control, and difficulties with emotion regulation.
Reward processing dysregulation
Neurobiological research has identified dysregulation in the brain’s reward circuitry as a core feature of BED. The dopaminergic reward system — which mediates the pleasure and motivation associated with food — shows altered responsivity in people with BED, producing heightened reward salience for food and reduced ability to inhibit food-seeking behavior in the presence of food cues or emotional distress (Medscape, 2025).
Impaired inhibitory control
The prefrontal cortical systems that mediate impulse control — the capacity to inhibit an appetitive response — show reduced function in individuals with BED. This impaired inhibitory control is the neurological mechanism that underlies the subjective loss of control that defines binge eating episodes (Medscape, 2025).
Emotion dysregulation
Binge eating frequently functions as an emotion regulation strategy — a way of managing, suppressing, or escaping negative emotional states including anxiety, loneliness, boredom, stress, and depression. Research consistently shows that negative affect precedes binge eating episodes (affect regulation model) and that the eating provides temporary relief that reinforces the pattern. This relationship with emotion is one of the most consistently documented features of BED (Medscape, 2025; Frontiers in Psychiatry, 2022).
Cognitive features — weight and shape overvaluation
Internalized weight bias and overvaluation of body shape and weight as measures of self-worth are documented cognitive contributors to BED maintenance. These cognitions amplify post-episode shame and guilt, driving the negative affect cycle that maintains the disorder (Medscape, 2025; ScienceDirect evaluation of DSM-5 severity, 2015).
Genetic and familial factors
BED shows significant familial aggregation, suggesting genetic contributions to the neurobiological vulnerabilities underlying the disorder. First-degree relatives of individuals with BED have elevated rates of eating disorders and mood disorders.
History of dieting and weight stigma
Restrictive dieting — particularly in childhood or adolescence — is a documented risk factor for binge eating. The experience of weight stigma, which is disproportionately experienced by people in larger bodies, produces the chronic stress and negative affect that can activate and maintain BED.
Comorbidities
BED has very high psychiatric comorbidity rates. A community sample study (Psychiatrist.com, 2021) found that individuals meeting DSM-5 criteria for BED were significantly more likely to report lifetime depression (OR=3.82), lifetime anxiety (OR=3.17), lifetime bipolar disorder (OR=3.92), and ADHD in the last 6 months (OR=8.24) compared to those who did not meet BED criteria. A Frontiers in Psychiatry (2022) expert consensus study identified depression (prevalence 23.9–69.9%) and anxiety (55.5–65.1%) as the most consistently recognized comorbidities.
How This Test Works
This Binge Eating Disorder Test covers the complete DSM-5-TR diagnostic framework for BED across 15 questions — all five Criterion B behavioral features, Criterion A (loss of control and quantity), Criterion C (distress), Criterion D (frequency and duration), and the functional impact of the disorder on daily life and relationships.
Answer based on your consistent experience over the past 3 months — the time frame specified in DSM-5-TR Criterion D.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Total range: 0–60. This is a screening tool. It cannot diagnose BED — only a qualified clinician can do that through comprehensive assessment. If your score suggests significant BED patterns, the next step is speaking with a healthcare provider or eating disorder specialist.
Understanding Your BED Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few BED Indicators | Responses suggest few significant BED patterns. Occasional overeating or emotional eating may be present without a pattern consistent with Binge Eating Disorder. |
| 16 – 30 | Mild — Some BED Patterns Present | Some binge eating patterns are present. May not reach full BED threshold but warrants professional discussion and support around eating and emotional regulation. |
| 31 – 45 | Moderate — Significant BED Pattern | Significant binge eating pattern across multiple criteria. Consistent with BED; professional evaluation and support are recommended. |
| 46 – 60 | High — Strong BED Indicators | Pervasive and severe binge eating patterns across most domains. Professional evaluation and specialized eating disorder treatment are strongly recommended. |
Treatment for Binge Eating Disorder
BED is a treatable condition with strong evidence for several interventions. According to the Merck Manual (2026) and the most recent review by Dr. Carlos Grilo (Annual Review of Clinical Psychology, 2024), effective treatments include:
Cognitive Behavioral Therapy (CBT) — first-line
The most evidence-supported treatment for BED. CBT for BED specifically targets: (1) the behavioral patterns maintaining binge eating (irregular eating, dietary restriction, food avoidance) through behavioral regulation strategies; (2) the cognitive distortions around eating, body shape, and weight that fuel the shame cycle; and (3) the emotion regulation deficits that make binge eating a functional strategy for managing distress. CBT produces significant reductions in binge eating frequency, associated psychological features, and depression. It does not reliably produce weight loss but does prevent future weight gain (Grilo, 2024).
Interpersonal Psychotherapy (IPT)
An effective alternative to CBT that targets the interpersonal contexts that trigger and maintain binge eating — relationship difficulties, role transitions, grief, and interpersonal deficits. IPT is particularly indicated when clear interpersonal triggers for binge episodes are identifiable.
Dialectical Behavior Therapy (DBT)
Originally developed by Dr. Marsha Linehan for BPD, DBT is effective for BED given its specific emphasis on emotional regulation, distress tolerance, and mindfulness. For individuals where emotion dysregulation is the primary driver of binge eating, DBT provides targeted skills that address the mechanism directly.
Lisdexamfetamine (Vyvanse) — FDA-approved
The only medication specifically FDA-approved for moderate-to-severe BED. A stimulant medication (prodrug of dextroamphetamine) that reduces binge eating through its effects on impulse control and reward processing. Randomized double-blind placebo-controlled trials by Dr. Carlos Grilo and colleagues (2024) demonstrated a significant reduction in binge eating days with lisdexamfetamine maintenance treatment. Used alongside CBT for the strongest outcomes.
SSRIs (Selective serotonin reuptake inhibitors)
Reduce binge eating frequency and improve mood in BED. Not FDA-approved specifically for BED but widely used adjunctively, particularly when comorbid depression or anxiety is present.
Frequently Asked Questions
What is Binge Eating Disorder?
Binge Eating Disorder (BED) is a Feeding and Eating Disorder (DSM-5-TR; ICD-10-CM F50.81x) characterized by recurrent episodes of eating objectively large amounts of food with a felt loss of control, in the absence of compensatory behaviors, occurring at least once weekly for 3 months, associated with ≥3 of 5 behavioral features, and causing marked distress. It is the most common eating disorder in the United States and Western Europe (Hudson et al., 2007), affecting an estimated 2.5% of adults, with a mean age of onset of approximately 25.4 years. It was first described by Dr. Albert Stunkard in 1959 and received formal DSM-5 diagnosis status in 2013.
Is BED different from bulimia nervosa?
Yes — the critical difference is the absence of compensatory behaviors. In bulimia nervosa, binge eating episodes are followed by recurrent inappropriate compensatory behaviors — purging, excessive exercise, fasting, or laxative use — aimed at preventing weight gain. In BED, there are no such compensatory behaviors (DSM-5-TR Criterion E). Both disorders involve binge eating with loss of control, but bulimia nervosa is defined by the purge-binge cycle and BED is not. Treatment approaches have overlapping but distinct elements. If compensatory behaviors are present, please take the Eating Disorder Test for a more complete assessment.
Can people with BED be of normal or low weight?
Yes. BED occurs across the entire weight spectrum — in people of low, normal, and higher weights. Body weight is not a diagnostic criterion for BED and is not a reliable indicator of its presence or severity. The association between BED and higher body weight exists at a population level — BED is more prevalent among people seeking obesity treatment (approximately 14% in clinical obesity samples) — but a significant proportion of people with BED are in the normal or lower weight range. Assuming BED only affects people in larger bodies is one of the most significant barriers to recognition and diagnosis across the weight spectrum.
What is the relationship between BED and emotional eating?
Emotional eating — eating in response to emotional states rather than physical hunger — is common and is not itself a diagnosable condition. BED has significant overlap with emotional eating in that negative affect (anxiety, loneliness, stress, boredom, depression) is a documented trigger for binge eating episodes in BED. However, not all emotional eating constitutes BED — the diagnostic requirements include objectively large quantities, felt loss of control, specific behavioral features, marked distress, and a frequency/duration threshold. The presence of the emotional eating pattern is clinically significant in BED because it means the binge eating is functioning as an emotion regulation strategy, which is an important treatment target.
Is BED related to ADHD?
Research documents a significant association. A community sample study found that individuals meeting DSM-5 BED criteria were 8.24 times more likely to have ADHD in the past 6 months compared to those without BED (Psychiatrist.com, 2021). The WHO World Mental Health Surveys found the highest comorbidity association between lifetime BED and lifetime ADHD of any psychiatric comorbidity assessed (Frontiers in Psychiatry, 2022). The overlap likely reflects shared neurobiological features — impaired impulse control and reward processing dysregulation are central to both conditions. Where ADHD is present alongside BED, treating the ADHD may reduce binge eating as a downstream effect. The ADHD Test is worth completing alongside this assessment.
Can BED be treated?
Yes — BED has a strong evidence base for treatment. CBT is the first-line psychological treatment and produces significant, robust reductions in binge eating frequency and associated psychological features (Grilo, 2024). Interpersonal Psychotherapy (IPT) and Dialectical Behavior Therapy (DBT) are effective alternatives. Lisdexamfetamine (Vyvanse) is the only FDA-approved medication specifically for moderate-to-severe BED and demonstrates significant efficacy in randomized controlled trials. Despite effective treatments existing, only 43.6% of people with BED ever seek eating disorder-specific treatment (NIMH, NCS-R) — making awareness, destigmatization, and access to care the most critical barriers to address.
Where can I find support for Binge Eating Disorder?
The National Alliance for Eating Disorders helpline is available at 1-866-662-1235 (Monday–Friday, 9am – 5pm ET) and can help connect you with a specialist, provide information about treatment options, and offer support. For after-hours crisis support, text NEDA to 741741 (Crisis Text Line). For clinical treatment, look for a therapist or psychologist with specific training in eating disorders and CBT for BED — this specialization matters for treatment efficacy.
Related Tests
- Eating Disorder Test — broader eating disorder screening covering anorexia, bulimia, and BED patterns; important if compensatory behaviors are also present
- Clinical Depression Test — depression is the most common BED comorbidity (prevalence 23.9–69.9%); it needs to be assessed and treated separately
- Anxiety Test — anxiety disorders are the second most common BED comorbidity (55.5–65.1%); anxiety is a major trigger for binge episodes
- ADHD Test — ADHD has the highest comorbidity association with BED of any psychiatric disorder in WHO surveys; shared impulsivity mechanisms
- Bipolar Test — bipolar disorder is significantly elevated in BED (OR=3.92); mood cycling can drive binge eating episodes
- Anhedonia Test — loss of the capacity for pleasure is a depression feature commonly co-occurring with BED
- Dysthymia Test — persistent low-grade depression frequently co-occurs with BED and can be a chronic trigger for binge episodes
- PTSD Test — trauma history is a documented risk factor for BED; PTSD and BED frequently co-occur
- Imposter Syndrome Test — shame-driven concealment is a shared feature of BED and imposter syndrome; worth exploring if self-worth concerns are prominent
For more eating-disorder and mental-health assessments, visit our Mental Health collection.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Binge-Eating Disorder (F50.81x), pp. 392–396. psychiatry.org
- Hudson, J.I., Hiripi, E., Pope, H.G. Jr., & Kessler, R.C. (2007). The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry, 61(3), 348–358. [Women 3.5%, men 2.0%; ADHD comorbidity] pubmed.ncbi.nlm.nih.gov
- Grilo, C.M. (2024). Treatment of Eating Disorders: Current Status, Challenges, and Future Directions. Annual Review of Clinical Psychology, 20(1), 97–123. annualreviews.org
- Grilo, C.M., Ivezaj, V., Yurkow, S., et al. (2024). Lisdexamfetamine maintenance treatment for binge-eating disorder following successful treatments: randomized double-blind placebo-controlled trial. Psychological Medicine, 54(12), 1–11. pubmed.ncbi.nlm.nih.gov
- Merck Manual Professional Edition. (2026). Binge-Eating Disorder. Reviewed/Revised Aug 2025. merckmanuals.com
- Medscape. (2025). Binge Eating Disorder: Background, Diagnostic Criteria, Epidemiology. emedicine.medscape.com
- National Institute of Mental Health (NIMH). (2024). Eating Disorders Statistics. National Comorbidity Survey Replication (NCS-R) data. [Past-year prevalence 1.2%; onset 21 years; 43.6% treatment-seeking] nimh.nih.gov
- Kimber, M., Szatmari, P., et al. (2021). Estimating the prevalence of binge eating disorder in a community sample from the United States: Comparing DSM-IV-TR and DSM-5 criteria. [Depression OR=3.82, anxiety OR=3.17, bipolar OR=3.92, ADHD OR=8.24] Journal of Clinical Psychiatry. psychiatrist.com
- Lydecker, J.A., et al. (2022). Mental health aspects of binge eating disorder: cross-sectional mixed-methods study of expert perspectives. Frontiers in Psychiatry. [Depression 23.9–69.9%; anxiety 55.5–65.1%; ADHD highest WHO comorbidity] frontiersin.org
- National Alliance for Eating Disorders. Helpline: 1-866-662-1235. allianceforeatingdisorders.com
- Wikipedia. (2025). Binge eating disorder. en.wikipedia.org