
The flaw feels enormous — undeniable, glaring, the first thing anyone would notice. So it can be genuinely disorienting when others say they don’t see it, or insist it looks completely normal. That gap between what you see in the mirror and what everyone else sees is the central, defining experience of Body Dysmorphic Disorder (BDD). It is not vanity. It is not a failure of perspective; you should simply be able to correct. It is a recognized psychiatric condition involving a real disturbance in how appearance is perceived and processed — and it can consume hours of every day.
BDD affects an estimated 1.7% to 2.9% of people — more common than anorexia or schizophrenia, and roughly as common as OCD (Phillips, International OCD Foundation). Yet only about 15% of people with BDD seek treatment specifically for it, partly because the shame is so acute and partly because BDD is so often misdiagnosed as depression or social anxiety (Conroy et al., 2008). It is also among the most dangerous conditions in psychiatry: roughly 80% of people with BDD experience suicidal thoughts, and 24-28% attempt suicide at least once (Phillips, 2007). This is why recognizing it matters so much.
This free Body Dysmorphic Disorder Test screens for BDD using the DSM-5-TR diagnostic criteria (APA, 2022), informed by the BDDQ and BDD-YBOCS clinical instruments developed by Dr. Katharine Phillips. 12 questions. Instant, private results.
What Is Body Dysmorphic Disorder?
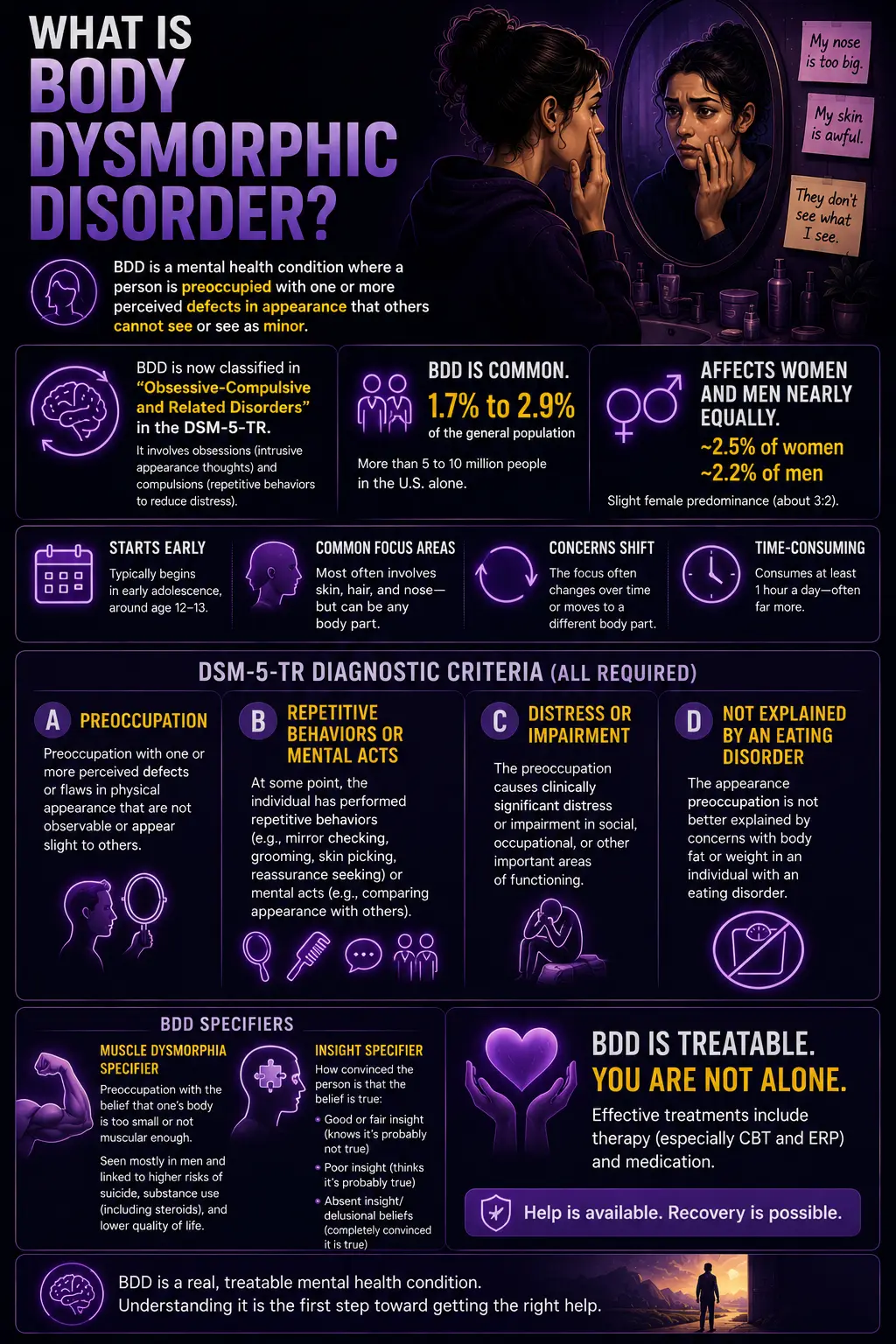
Body Dysmorphic Disorder (BDD) — DSM-5-TR code 300.7 (F45.22) — is a mental health condition characterized by preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear only slight to others. The preoccupation is time-consuming (typically occupying at least an hour a day, often far more), causes significant distress or impairment, and drives repetitive behaviors — mirror checking, grooming, skin picking, reassurance seeking, or comparing one’s appearance to others (APA, 2022).
One of the most significant changes in the DSM-5 (2013, carried into the DSM-5-TR) was the reclassification of BDD. Previously grouped with the somatoform disorders (DSM-IV), BDD was moved into the new category of “Obsessive-Compulsive and Related Disorders”, alongside OCD, hoarding disorder, trichotillomania, and excoriation (skin-picking) disorder (Schieber et al., 2015). This reflects the clinical reality of BDD: the appearance preoccupations function like obsessions (intrusive, distressing, hard to resist), and the checking and concealing behaviors function like compulsions (repetitive, performed to reduce distress). The DSM-5 also added a new diagnostic requirement — Criterion B — explicitly requiring the presence of these repetitive behaviors or mental acts.
BDD affects an estimated 1.7% to 2.9% of the general population — more than 5 to 10 million people in the United States alone (Phillips, IOCDF). It affects women and men nearly equally (approximately 2.5% of women and 2.2% of men), with a slight female predominance of roughly 3:2 (DSM-5-TR). BDD typically begins in early adolescence, around age 12-13 (Phillips; Bjornsson, 2017), though it is frequently not diagnosed until years or decades later. The body areas of concern most commonly involve the skin, hair, and nose — but BDD can focus on any body part, and concerns frequently shift over time.
The full DSM-5-TR diagnostic criteria for BDD (all required; APA, 2022):
- Criterion A: Preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others.
- Criterion B: At some point during the course of the disorder, the individual has performed repetitive behaviors (e.g., mirror checking, excessive grooming, skin picking, reassurance seeking) or mental acts (e.g., comparing their appearance with that of others) in response to the appearance concerns.
- Criterion C: The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- Criterion D: The appearance preoccupation is not better explained by concerns with body fat or weight in an individual whose symptoms meet diagnostic criteria for an eating disorder.
The DSM-5-TR includes two specifiers. The muscle dysmorphia specifier applies when the preoccupation centers on the idea that one’s body build is too small or insufficiently muscular — a form seen predominantly in men, associated with even higher rates of suicidality, substance use (including anabolic steroids), and poorer quality of life. The insight specifier indicates how convinced the person is that their belief is true: good or fair insight (recognizes the belief is probably not true), poor insight (thinks it is probably true), or absent insight/delusional beliefs (completely convinced it is true).
Signs You Might Have Body Dysmorphic Disorder
BDD is one of the most under-recognized conditions in mental health — frequently hidden out of shame, and frequently misdiagnosed because the person presents with depression or social anxiety that BDD produces rather than the appearance preoccupation itself. These are the signs that most reliably distinguish BDD from ordinary appearance concerns.
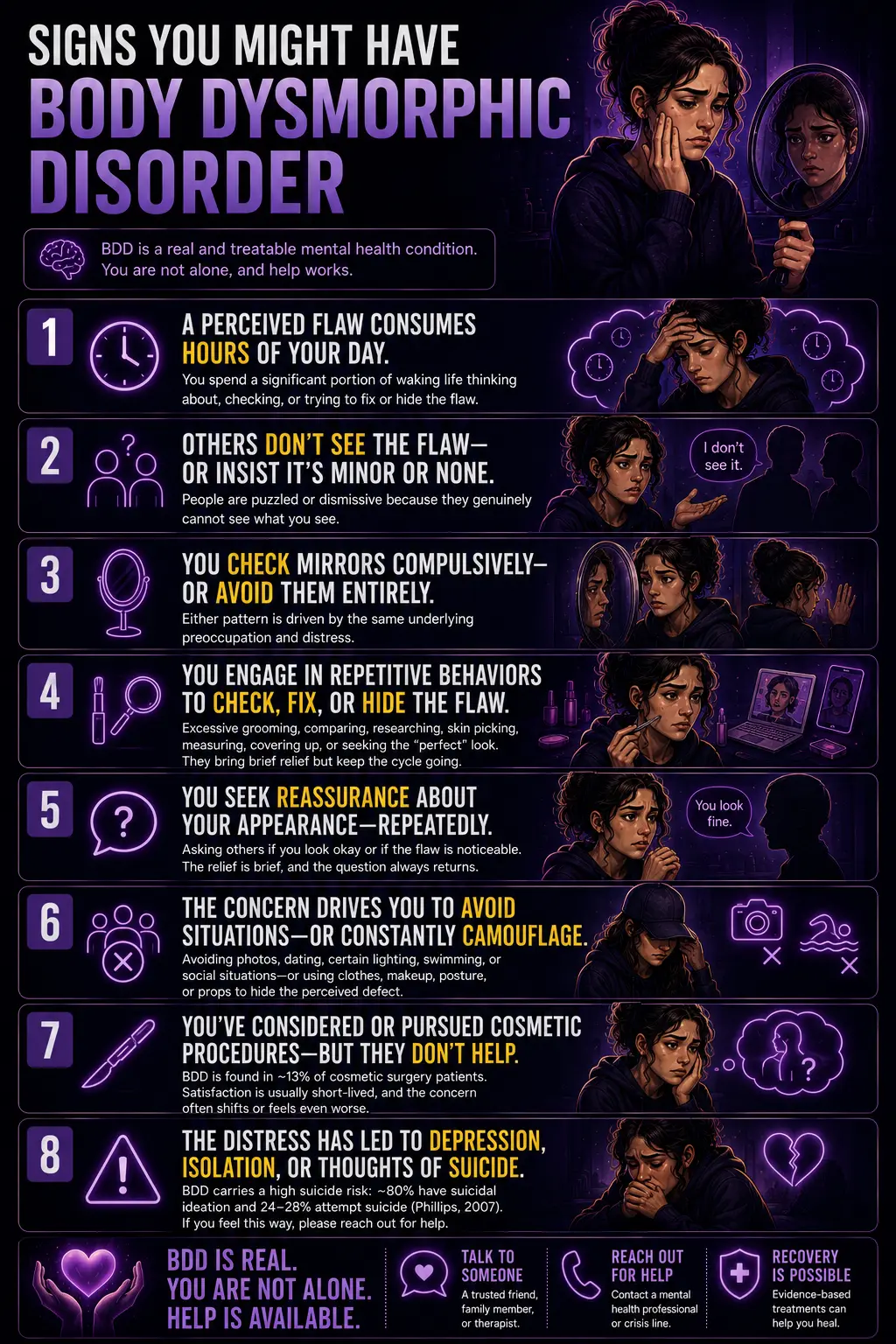
A perceived flaw consumes hours of your day. The clinical threshold for “preoccupation” is typically about an hour a day, but for many people with BDD, it is far more — a significant portion of waking life spent thinking about, checking, or trying to fix or hide the perceived flaw. This is the feature that most clearly separates BDD from normal insecurity: the sheer quantity of time and mental energy the concern consumes.
Others don’t see the flaw — or insist it’s minor or nonexistent. The hallmark of BDD is the gap between perception and reality. When you raise the concern, people are puzzled, reassuring, or dismissive — not because they’re being kind, but because they genuinely cannot see what you see. The reassurance doesn’t land because the flaw feels so obviously, glaringly real to you.
You check mirrors compulsively — or avoid them entirely. BDD produces two opposite but related behaviors around mirrors. Some people check repeatedly — drawn back again and again to scrutinize, measure, and assess the flaw. Others avoid mirrors, reflective surfaces, and photos entirely because seeing the flaw is too distressing. Both patterns are driven by the same underlying preoccupation.
You engage in repetitive behaviors to check, fix, or hide the flaw. Excessive grooming, skin picking, applying makeup to cover, styling hair to conceal, changing clothes repeatedly, measuring or touching the body part, researching procedures, or comparing your appearance to other people’s (in person, in photos, on social media). These behaviors temporarily reduce anxiety but reinforce the preoccupation over time — the compulsion half of the obsessive-compulsive pattern.
You seek reassurance about your appearance — repeatedly. Asking others whether you look okay, whether the flaw is noticeable, and whether a procedure helped. The reassurance provides brief relief but never lasts, so the question returns. Reassurance-seeking is one of the most recognizable BDD behaviors and one of the most straining on relationships.
The concern drives you to avoid situations — or to constantly camouflage. Avoiding social situations, dating, photographs, certain lighting, swimming, or any context where the flaw might be exposed or scrutinized. When you can’t avoid, you camouflage — hats, makeup, clothing, posture, hand position — to hide the perceived defect. The avoidance and camouflage can severely restrict daily life.
You’ve considered or pursued cosmetic procedures — but they don’t resolve the distress. Many people with BDD seek cosmetic, dermatological, or surgical procedures to fix the perceived flaw. BDD is found in roughly 13% of cosmetic surgery patients (Angelakis et al., 2016). Critically, these procedures rarely help — the satisfaction is usually short-lived, the concern often shifts to another body part, or the person becomes distressed that the procedure “made it worse.” BDD is a perceptual and psychological condition; it does not resolve through physical alteration.
The distress has led to depression, isolation, or thoughts of suicide. BDD carries one of the highest suicide risks in psychiatry — approximately 80% experience suicidal ideation and 24-28% attempt suicide (Phillips, 2007). If your appearance concerns have led to hopelessness, withdrawal from people you care about, or thoughts that life isn’t worth living, this is a sign of how serious BDD is — and a reason to reach out for help now, not later.
BDD vs OCD vs Eating Disorders vs Social Anxiety
| Feature | Body Dysmorphic Disorder | OCD | Eating Disorders | Social Anxiety Disorder |
|---|---|---|---|---|
| Core preoccupation | Specific perceived flaw(s) in physical appearance | Varied obsessions (contamination, harm, symmetry, etc.) | Body weight, shape, and food/eating | Being negatively judged or embarrassing oneself socially |
| Repetitive behaviors | Mirror checking, grooming, camouflaging, reassurance seeking, comparing | Compulsions (washing, checking, counting, ordering) | Restriction, bingeing, purging, body checking | Avoidance, safety behaviors in social situations |
| DSM-5-TR category | Obsessive-Compulsive and Related Disorders | Obsessive-Compulsive and Related Disorders (same family) | Feeding and Eating Disorders | Anxiety Disorders |
| Key distinction | Appearance flaw is the focus; if concern is ONLY weight/fat with an eating disorder, that’s the ED diagnosis (Criterion D) | Obsessions are usually not about appearance; if they are, BDD is the better fit | Focus is weight/shape and eating behavior, not a specific non-weight appearance flaw | Fear is about social judgment generally, not driven by a specific perceived physical defect |
| Insight | Often poor or absent, many are convinced the flaw is real (delusional in some cases) | Usually, better insight — most recognize obsessions are excessive | Variable: body image disturbance can be severe | Usually intact — aware that the fear is disproportionate |
| PsyMed test | This test | OCD Test | Anorexia Test / BED Test | Social Anxiety Test |
The BDD/eating disorder distinction is the most clinically important because they overlap heavily, and the DSM-5-TR addresses it directly in Criterion D. If appearance concerns are exclusively about being fat or about body weight in someone who meets criteria for an eating disorder, the eating disorder diagnosis takes precedence. But BDD frequently focuses on non-weight features (skin, nose, hair, symmetry, a specific body part), and the two conditions can co-occur. Muscle dysmorphia — the BDD subtype involving preoccupation with being insufficiently muscular — sits at this intersection and is sometimes confused with an eating disorder, but it is classified as a form of BDD.
Understanding Your Body Dysmorphic Disorder Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 12 | Minimal — Few BDD Indicators | A few signs of body dysmorphic disorder. Normal appearance concerns may be present without the time consumption, repetitive behaviors, or impairment that characterize BDD. |
| 13 – 24 | Mild — Some BDD Features | Some BDD features are present. Appearance concerns may be taking up meaningful time and prompting checking or comparing behaviors. Worth monitoring and discussing with a professional. |
| 25 – 36 | Moderate — Significant BDD Indicators | Significant indicators consistent with BDD. The preoccupation, repetitive behaviors, and impairment are likely affecting daily life. Professional evaluation is recommended. |
| 37 – 48 | High — Strong BDD Indicators | Strong indicators of BDD across multiple criteria. The condition is very likely significantly affecting functioning and well-being. Professional evaluation and treatment are strongly recommended. |
What Causes Body Dysmorphic Disorder?
BDD develops from an interaction of biological, psychological, and environmental factors, consistent with its classification in the OCD spectrum.
Neurobiological factors. BDD shows abnormalities in visual processing — research suggests people with BDD have a bias toward detailed, local processing of faces and appearance (focusing on specific features) rather than holistic, global processing. This may underlie the experience of fixating on a single perceived flaw rather than perceiving the face as a whole. The serotonergic system is implicated, consistent with BDD’s response to SSRIs. BDD shares neurobiological features with OCD, including involvement of fronto-striatal circuits.
Genetic factors. BDD has a heritable component — it runs in families and shows elevated rates among first-degree relatives, including overlap with OCD. A population-based twin study of over 15,000 adolescents and young adults found significant heritability of body dysmorphic concerns (Cambridge, Psychological Medicine, 2018).
Psychological and developmental factors. Adverse childhood experiences — including teasing or bullying about appearance, abuse, and neglect — are documented risk factors for BDD (Angelakis et al.). Perfectionism, high aesthetic sensitivity, and a tendency toward internalizing self-criticism are associated personality features. Low self-esteem and a self-worth heavily contingent on appearance increase vulnerability.
Sociocultural factors. Cultural emphasis on appearance, idealized and digitally altered images, and social media’s intensification of appearance comparison all interact with underlying vulnerability. Social media in particular provides both an endless stream of comparison targets and tools (filters, editing) that can intensify the gap between perceived and idealized appearance.
Treatment for Body Dysmorphic Disorder
BDD is treatable, and this is the most important message for anyone whose result raises concern. The first two lines of evidence-based treatments are CBT specifically adapted for BDD and SSRI medication.
Cognitive Behavioral Therapy for BDD (CBT-BDD). CBT specifically tailored for BDD is the gold-standard psychological treatment, showing 50-80% symptom reduction (research summaries). CBT-BDD includes: cognitive restructuring of appearance-related beliefs; exposure and response prevention (reducing checking, camouflaging, and reassurance-seeking); perceptual retraining (mirror work that builds holistic rather than detail-focused viewing); and relapse prevention. The approach was developed by clinicians, including Dr. Sabine Wilhelm, Dr. Katharine Phillips, and Dr. David Veale.
Medication — SSRIs. Selective serotonin reuptake inhibitors are the first-line medication for BDD and are effective in approximately 63% of patients. BDD often requires higher SSRI doses and longer trials (12-16 weeks) than depression. SSRIs reduce the preoccupation, distress, and compulsive behaviors, and lower suicidality. For severe or treatment-resistant cases, combined CBT and SSRI treatment is recommended.
What does not work: cosmetic procedures. This is critical. Cosmetic, surgical, and dermatological procedures do not treat BDD and frequently make it worse — satisfaction is brief, the concern shifts to another feature, or the person becomes distressed about the result. Major clinical guidelines advise against cosmetic intervention as a treatment for BDD. The condition is perceptual and psychological; it responds to psychological and pharmacological treatment, not physical alteration.
Frequently Asked Questions
What is body dysmorphic disorder?
Body Dysmorphic Disorder (BDD; DSM-5-TR 300.7 / F45.22) is a mental health condition characterized by preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear only slight to others. The preoccupation is time-consuming (typically an hour or more per day), causes significant distress or impairment, and is accompanied by repetitive behaviors such as mirror checking, grooming, camouflaging, reassurance seeking, or comparing one’s appearance to others. In the DSM-5, BDD is classified among the Obsessive-Compulsive and Related Disorders. It affects 1.7-2.9% of the population and typically begins around age 12-13.
Is body dysmorphia the same as being insecure about your looks?
No. Ordinary insecurity about appearance is common and usually manageable — it doesn’t consume hours a day, doesn’t drive compulsive checking or concealing behaviors, and doesn’t cause significant impairment in daily functioning. BDD is a clinical disorder defined by the intensity, time consumption, and impairment involved. The key distinctions: the perceived flaw is not visible or appears only slight to others; the preoccupation occupies a significant portion of the day; it drives repetitive behaviors; and it causes clinically significant distress or interferes with work, relationships, or daily life. BDD also carries serious risks — roughly 80% experience suicidal ideation — that ordinary insecurity does not.
What body parts does BDD usually focus on?
BDD can focus on any body part, and concerns frequently shift over time. The most common areas are the skin (acne, scarring, complexion, perceived blemishes), hair (thinning, texture, body hair), and nose (shape, size). Other common concerns include the eyes, teeth, jaw, chin, facial asymmetry, and overall facial features. The muscle dysmorphia subtype focuses on the idea that one’s body build is too small or insufficiently muscular, seen predominantly in men. Many people with BDD are preoccupied with several body areas, either simultaneously or shifting over time.
Is body dysmorphic disorder an eating disorder?
No, though they overlap and can co-occur. BDD is classified among the Obsessive-Compulsive and Related Disorders, while eating disorders are a separate DSM-5-TR category (Feeding and Eating Disorders). The DSM-5-TR addresses the distinction directly in BDD Criterion D: if appearance concerns are exclusively about being fat or about body weight in someone who meets criteria for an eating disorder, the eating disorder diagnosis applies. BDD typically focuses on non-weight features (skin, nose, hair, a specific body part). The two can co-occur, and muscle dysmorphia (a BDD subtype) sits near this boundary but is classified as BDD. If your concerns center on weight, shape, and eating behaviors, the Anorexia Test or Binge Eating Disorder Test may be more relevant.
Why is BDD considered related to OCD?
In the DSM-5 (2013), BDD was moved from the somatoform disorders into the new category of “Obsessive-Compulsive and Related Disorders,” alongside OCD, hoarding disorder, trichotillomania, and excoriation disorder. The reasoning: BDD’s appearance preoccupations function like obsessions (intrusive, distressing, persistent, difficult to resist), and its checking, grooming, camouflaging, and reassurance-seeking behaviors function like compulsions (repetitive, performed to reduce distress). BDD and OCD also share neurobiological features, run together in families, and respond to similar treatments (SSRIs and exposure-based CBT). The DSM-5 added Criterion B specifically to require the presence of these repetitive behaviors. The OCD Test screens for the broader obsessive-compulsive pattern.
Can body dysmorphic disorder be treated?
Yes — BDD is treatable. The first two lines of evidence-based treatments are Cognitive Behavioral Therapy specifically adapted for BDD (CBT-BDD), which shows 50-80% symptom reduction, and SSRI medication, effective in approximately 63% of patients. CBT-BDD includes cognitive restructuring, exposure, and response prevention (reducing checking and camouflaging), and perceptual retraining. BDD often requires higher SSRI doses and longer trials than depression. Importantly, cosmetic and surgical procedures do not treat BDD and frequently worsen it — the condition is perceptual and psychological, and responds to psychological and pharmacological treatment, not physical alteration. With proper treatment, most people experience meaningful improvement.
How is BDD diagnosed?
BDD is diagnosed by a qualified mental health professional using the DSM-5-TR criteria through clinical interview. The validated instruments include the Body Dysmorphic Disorder Questionnaire (BDDQ), a brief self-report screening tool developed by Dr. Katharine Phillips, and the Yale-Brown Obsessive Compulsive Scale Modified for BDD (BDD-YBOCS; Phillips et al., 1997), a clinician-administered scale that measures severity, where a score of 20 or above indicates clinically significant BDD. Diagnosis requires all four criteria: appearance, preoccupation with flaws not observable or slight to others (A); repetitive behaviors or mental acts in response (B); clinically significant distress or impairment (C); and the preoccupation not being better explained by an eating disorder (D). This Body Dysmorphic Disorder test is a screening tool, not a diagnosis; only a professional can diagnose BDD.
Related Tests
- OCD Test — BDD is classified in the OCD spectrum; the two share obsessive-compulsive mechanisms, run together in families, and respond to similar treatments
- Anorexia Test — eating disorders overlap with BDD; the distinction hinges on whether concerns are weight/shape-focused or about a specific non-weight appearance flaw
- Binge Eating Disorder Test — body image disturbance is common across eating and body-image conditions; worth assessing if eating behaviors are involved
- Social Anxiety Test — BDD frequently produces social avoidance and is often misdiagnosed as social anxiety; the two commonly co-occur
- Clinical Depression Test — about 90% of people with BDD experience a major depressive episode; depression is the most common comorbidity and the most common misdiagnosis
- Anxiety Test — anxiety disorders commonly co-occur with BDD; the chronic appearance-related worry overlaps with generalized anxiety
- Self-Esteem Test — appearance-contingent self-worth is a core vulnerability in BDD; low self-esteem both contributes to and results from the disorder
- Depersonalization Disorder Test — distorted self-perception appears in both conditions; worth distinguishing if the experience involves feeling detached from one’s body or appearance
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Body Dysmorphic Disorder 300.7 (F45.22). psychiatry.org
- Phillips, K.A., et al. (1997). A severity rating scale for body dysmorphic disorder: development, reliability, and validity of a modified version of the Yale-Brown Obsessive Compulsive Scale (BDD-YBOCS). Psychopharmacology Bulletin, 33(1), 17–22. [BDD-YBOCS; alpha=.80; ≥20 clinical threshold]
- Phillips, K.A. (2007). Suicidality in Body Dysmorphic Disorder. Primary Psychiatry, 14(12), 58–66. PMC2361388. [~80% suicidal ideation; 24-28% attempt] pmc.ncbi.nlm.nih.gov
- Angelakis, I., Gooding, P.A., & Panagioti, M. (2016). Suicidality in body dysmorphic disorder (BDD): A systematic review with meta-analysis. Clinical Psychology Review, 49, 55–66. [Suicide attempt OR=3.30; ideation OR=2.57; 13% cosmetic surgery prevalence] sciencedirect.com
- Rief, W., Buhlmann, U., Wilhelm, S., et al. (2006). The prevalence of body dysmorphic disorder: a population-based survey. Psychological Medicine, 36(6), 877–885. [Prevalence 1.7%] pubmed.ncbi.nlm.nih.gov
- Schieber, K., Kollei, I., de Zwaan, M., & Martin, A. (2015). Classification of body dysmorphic disorder — What is the advantage of the new DSM-5 criteria? Journal of Psychosomatic Research, 78(3), 223–227. [DSM-5 reclassification to OCD spectrum; Criterion B] sciencedirect.com
- Phillips, K.A. — International OCD Foundation. Prevalence and Diagnosis of BDD. [1.7-2.9% prevalence; DSM-5 criteria; specifiers] bdd.iocdf.org
- Enander, J., et al. (2018). Prevalence and heritability of body dysmorphic symptoms in adolescents and young adults: a population-based nationwide twin study. Psychological Medicine, 48(16). [N=15,377; heritability] cambridge.org
- Conroy, M., et al. (2008). Body dysmorphic disorder prevalence in inpatients. [BDD under-recognized; ~15% seek BDD-specific treatment; rarely identified without structured interview]