If you are in crisis right now, please reach out immediately.
📞 988 Suicide & Crisis Lifeline — Call or text 988 (United States, 24/7)
💬 Crisis Text Line — Text TALK to 741741
🌐 International resources: IASP Crisis Centers Directory
If you are in immediate danger, please go to your nearest emergency room or call emergency services.
There are thoughts that feel unspeakable — the kind that arrive unbidden and leave you wondering what they mean about you, about how much pain you are carrying, and about what to do next. Thoughts about not wanting to be here. Thoughts that range from a quiet wish to disappear to something more deliberate and specific. These thoughts are more common than most people realize, and their presence does not make you broken, dangerous, or beyond help. They are a signal — one that deserves to be taken seriously, understood clearly, and responded to with care.
This free suicidal ideation screening test is modeled on the clinical framework established by the Columbia Suicide Severity Rating Scale (C-SSRS), developed by Dr. Kelly Posner and colleagues at Columbia University, the University of Pennsylvania, and the University of Pittsburgh (Posner et al., 2011, American Journal of Psychiatry). The C-SSRS is the most widely validated instrument for assessing suicidal ideation severity and is endorsed by the U.S. Food and Drug Administration, the Centers for Disease Control and Prevention, and the World Health Organization.
This free suicidal test has 15 questions. Based on the past 2 weeks. Instant, private results — with clear guidance on what your score means and what to do next.
What Is Suicidal Ideation?
Suicidal ideation refers to thoughts about ending one’s own life, ranging in severity from passive wishes to no longer exist through to active planning with intent to act. The word “ideation” simply means thoughts — it does not imply action, inevitability, or certainty about what a person will do.
According to StatPearls (2024, NCBI Bookshelf), suicidal ideation is a critical mental health concern that can arise in individuals of any age or background, and is commonly associated with psychiatric conditions including depression, bipolar disorder, schizophrenia, and substance use disorders — but it is not exclusive to people with diagnosed conditions. It can emerge in the context of acute crisis, prolonged distress, hopelessness, and a sense of being a burden to others.
The World Health Organization estimates that approximately 700,000 people die by suicide each year globally (WHO, 2023). In the United States, the CDC’s 2023 Youth Risk Behavior Survey found that 20.4% of high school students had seriously considered attempting suicide in the past year. Among adults, the National Survey on Drug Use and Health (SAMHSA, 2022) found that approximately 12.3 million adults in the United States had serious thoughts about suicide in the past year.
These numbers exist not to alarm but to underscore something important: suicidal ideation is not rare, is not a sign of weakness or failure, and is not something you should carry alone. It is a recognized clinical experience with known risk factors, evidence-based treatments, and — critically — the capacity for meaningful improvement with appropriate support.

The C-SSRS Framework — Five Types of Suicidal Ideation
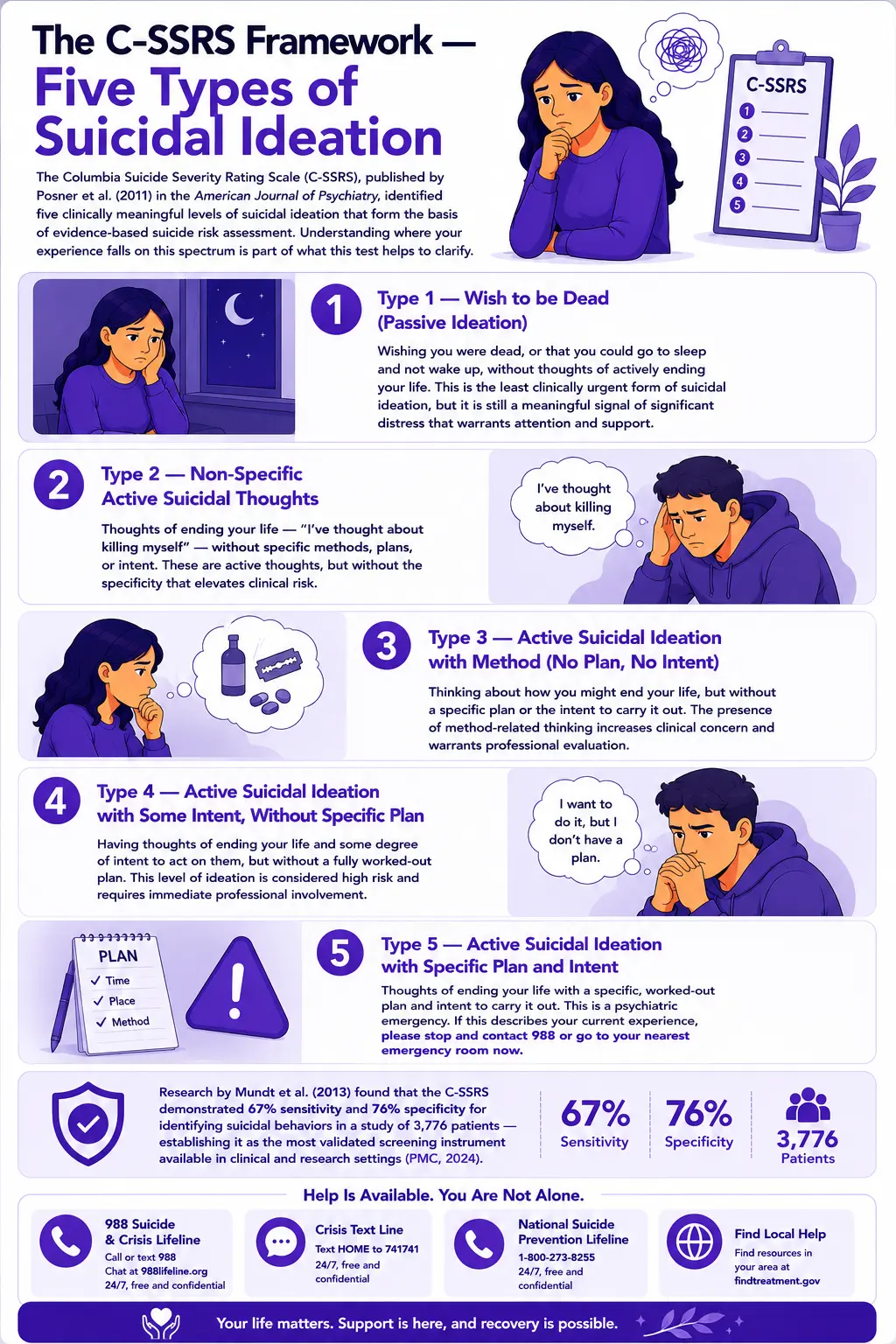
The Columbia Suicide Severity Rating Scale (C-SSRS), published by Posner et al. (2011) in the American Journal of Psychiatry, identified five clinically meaningful levels of suicidal ideation that form the basis of evidence-based suicide risk assessment. Understanding where your experience falls on this spectrum is part of what this test helps to clarify.
-
Wish to be Dead (Passive Ideation)
Wishing you were dead, or that you could go to sleep and not wake up, without thoughts of actively ending your life. This is the least clinically urgent form of suicidal ideation, but it is still a meaningful signal of significant distress that warrants attention and support.
-
Non-Specific Active Suicidal Thoughts
Thoughts of ending your life — “I’ve thought about killing myself” — without specific methods, plans, or intent. These are active thoughts, but without the specificity that elevates clinical risk.
-
Active Suicidal Ideation with Method (No Plan, No Intent)
Thinking about how you might end your life, but without a specific plan or the intent to carry it out. The presence of method-related thinking increases clinical concern and warrants professional evaluation.
-
Active Suicidal Ideation with Some Intent, Without Specific Plan
Having thoughts of ending your life and some degree of intent to act on them, but without a fully worked-out plan. This level of ideation is considered high risk and requires immediate professional involvement.
-
Active Suicidal Ideation with Specific Plan and Intent
Thoughts of ending your life with a specific, worked-out plan and intent to carry it out. This is a psychiatric emergency. If this describes your current experience, please stop and contact 988 or go to your nearest emergency room now.
Research by Mundt et al. (2013) found that the C-SSRS demonstrated 67% sensitivity and 76% specificity for identifying suicidal behaviors in a study of 3,776 patients — establishing it as the most validated screening instrument available in clinical and research settings (PMC, 2024).
Signs You May Be Experiencing Suicidal Ideation
Suicidal thoughts do not always announce themselves clearly. They can be subtle, ambiguous, and easily dismissed — including by the person experiencing them. These are the patterns that most consistently indicate suicidal ideation may be present and warrant attention:
-
Persistent thoughts about not wanting to exist
A recurring wish to disappear, to not wake up, or to no longer be here, without necessarily a specific plan or intention. These thoughts may feel passive or abstract, but they are not neutral. The persistence of a wish to no longer exist is a meaningful signal of serious distress, regardless of how specific or vague the thought is.
-
Increasing feelings of hopelessness — the sense that things will not get better
Hopelessness is one of the strongest predictors of suicidal ideation and behavior identified in research. A study published in PMC (2025) found that when hopelessness and depression occur together, they produce a 14.56-fold increase in suicidal ideation risk compared to the absence of both factors. If you have begun to believe that your situation is permanently unimprovable — not just hard right now, but impossible to change — that belief itself needs to be addressed as a clinical target.
-
Feeling like a burden to the people around you
The belief that others would be better off without you — that your absence would be a relief to your family, your partner, or your friends — is a specific and clinically significant cognitive pattern associated with elevated suicide risk. This belief is a distortion produced by the pain of depression and crisis, not an accurate assessment of your value to others.
-
Withdrawing from people and activities you previously cared about
Social withdrawal, loss of interest in relationships and activities, and increasing isolation are both signs of depression and behaviors that increase suicide risk by removing the social connections and protective relationships that buffer against crisis.
-
Giving away possessions, saying goodbye, or putting affairs in order without a clear reason
These behaviors — particularly in someone who has been expressing hopelessness or suicidal thoughts — are potential warning signs that should be taken seriously and addressed directly.
-
A sudden calm or improvement after a period of severe depression
Counterintuitively, a sudden lift in mood after a period of severe, hopeless depression can sometimes indicate that a person has made a decision about ending their life — the decision itself producing temporary relief from the anguish of ambivalence. This pattern warrants attention and inquiry rather than reassurance.
-
Increasing use of alcohol or substances during a period of distress
The CDC identifies substance use as a significant risk factor for suicidal behavior (CDC, 2024). Alcohol and other substances reduce inhibition and increase impulsivity — making it more likely that distress will translate into action during an acute crisis.
Risk Factors for Suicidal Ideation
Suicide is rarely caused by a single factor. The CDC (2024) identifies risk factors at the individual, relationship, community, and societal levels. Key individual risk factors include:
-
Previous suicide attempt
A prior attempt is the single strongest predictor of future suicidal behavior, according to the CDC (2024). This is not a reason for shame — it is a reason for sustained professional support and careful safety planning.
-
Mental health conditions
Depression, bipolar disorder, anxiety disorders, Borderline Personality Disorder, schizophrenia, and substance use disorders all significantly elevate suicide risk. StatPearls (2024) identifies these as the most consistently documented psychiatric risk factors for suicidal ideation.
-
Hopelessness
Aaron Beck’s foundational research established hopelessness as a mediator between depression and suicidal intent — more predictive of suicidal risk than depression severity alone. Research published in PMC (2025) confirmed that hopelessness and depression have an additive interaction, producing a 14.56-fold increase in suicidal ideation risk when both are present.
-
Chronic illness or pain
Serious illness, chronic pain, and conditions that significantly impair quality of life are associated with elevated suicidal ideation risk (StatPearls, 2024).
-
History of adverse childhood experiences
Trauma, abuse, neglect, and adverse childhood experiences (ACEs) are documented risk factors for both mental health conditions and suicidal ideation across the lifespan (CDC, 2024).
-
LGBTQ+ identity in an unsupportive environment
StatPearls (2024) identifies members of the LGBTQ+ community as a population with elevated suicide rates, particularly in the context of stigma, discrimination, and lack of family or social support. If this applies to you, the Trevor Project’s TrevorLifeline (1-866-488-7386) provides specific support.
Protective Factors — What Reduces Risk
Protective factors are conditions and resources that buffer against suicidal crisis and reduce risk — the presence of which is as clinically important to assess as the risk factors themselves. The CDC (2024) identifies key protective factors, including:
Strong connections to family, friends, and community. Access to mental health care. Effective coping and problem-solving skills. Reasons for living — including relationships, responsibilities, spiritual or religious beliefs, and future-oriented thinking. Restricted access to lethal means during periods of crisis. A sense of purpose or meaning.
Research on the Reasons for Living Inventory (Linehan et al.) has consistently found that the strength of reasons for living is a significant moderator of suicidal ideation — the stronger the reasons for living, the lower the ideation severity, even in the context of significant depression and hopelessness (Frontiers in Psychiatry, 2025).
About This Suicidal Ideation Test
This test is modeled on the clinical framework of the Columbia Suicide Severity Rating Scale (C-SSRS) and covers the domains most relevant to a self-administered suicidal ideation screening: ideation frequency and intensity, hopelessness, perceived burdensomeness, social connection, and the strength of protective factors, including reasons for living and sense of future.
Answer based on your experience over the past 2 weeks — the same time frame used by clinical tools, including the PHQ-9 and the C-SSRS screening version.
Standard questions (Q1–Q12):
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Protective factor questions (Q13–Q15) — scored in reverse:
- Always = 0
- Often = 1
- Sometimes = 2
- Rarely = 3
- Never = 4
Total range: 0–60. This is a screening tool. It cannot diagnose suicidal ideation, assess your personal risk level, or replace clinical evaluation. If you are in crisis or at risk, please use the crisis resources at the top of this page — do not wait for your test results.
Understanding Your Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Distress Indicators | Responses suggest few significant indicators of suicidal ideation or severe distress at this time. Continue to monitor your well-being and reach out if things change. |
| 16 – 30 | Moderate — Significant Emotional Distress | Responses suggest significant emotional distress. Speaking with a mental health professional is recommended. You do not have to be in crisis to ask for help. |
| 31 – 45 | High — Serious Distress Indicators | Responses suggest serious distress with significant indicators of suicidal ideation. Promptly speaking with a mental health professional is strongly recommended. |
| 46 – 60 | Severe — Please Reach Out Now | Responses suggest severe distress. Please contact 988 or go to your nearest emergency room. You do not have to face this alone. |
What to Do After Taking This Suicidal Ideation Test
If your score is in the Moderate range (16–30): Contact a mental health professional this week. Call or text 988 if you need to talk to someone now. Tell someone you trust what you have been experiencing.
If your score is in the High range (31–45): Contact a mental health professional today or go to an urgent care mental health service. Call or text 988 now if you need immediate support. Do not wait to see if things improve on their own.
If your score is in the Severe range (46–60): Please stop reading and contact 988 or emergency services right now. Your safety is the only priority.
For any score — if you have a plan: If you have thought about how you would end your life and have some intent to act on it, this is a psychiatric emergency, regardless of your overall score. Please contact 988 or go to your nearest emergency room immediately.
Frequently Asked Questions
Am I suicidal or just dramatic?
This question — one of the most frequently searched on this topic — deserves a direct and compassionate answer. The word “dramatic” implies that what you are feeling is an exaggeration of a real situation, performed for effect. Suicidal ideation is the opposite: it is an internal experience that most people hide, minimize, and carry in silence — often for a long time before telling anyone. If you are asking whether your thoughts are “real enough” to count, the answer is yes. You do not need to have a plan. You do not need to have intent. Passive suicidal ideation — a wish to not exist, to go to sleep and not wake up, to simply no longer be here — is clinically meaningful and deserves attention and care. The threshold for reaching out is not “I have a plan.” The threshold is “I am hurting, and I need support.” Both are real. Both deserve help.
What is the difference between passive and active suicidal ideation?
Passive suicidal ideation involves thoughts about not wanting to exist — wishing you were dead, hoping you won’t wake up — without thoughts of actively ending your life. Active suicidal ideation involves thoughts about ending your own life, which may range from general thoughts without a method to specific planning with intent to act. The C-SSRS (Posner et al., 2011) identifies five levels of ideation severity from passive through to active ideation with a specific plan and intent. Both passive and active ideation are clinically significant and warrant support — the distinction affects the urgency and nature of that support, not whether it is needed.
Does having suicidal thoughts mean I will act on them?
No. The vast majority of people who experience suicidal thoughts — including recurring and distressing ones — do not die by suicide. Suicidal ideation is a clinical experience that can be assessed, addressed, and treated. The presence of thoughts does not determine outcomes. What matters most is whether those thoughts are accompanied by intent, planning, access to means, and the absence of protective factors — and whether the person gets appropriate support. Having the thoughts does not make action inevitable. Getting help is what changes the trajectory.
Why are protective factors included in this test?
Suicide risk is not determined by risk factors alone — protective factors are equally important clinical variables. Research consistently shows that the strength of reasons for living, quality of social connection, access to mental health care, and future-oriented thinking all buffer significantly against suicidal crisis (Linehan Reasons for Living Inventory; CDC Risk and Protective Factors, 2024). A test that measures only distress and ideation without assessing the resources that protect against it would produce an incomplete picture. Questions about reasons for living, support systems, and hope for the future are clinically meaningful and are included in evidence-based risk assessment tools, including the C-SSRS.
What should I do if someone I care about might be suicidal?
Ask them directly. Research consistently shows that asking someone directly whether they are having thoughts of suicide does not increase risk and frequently provides relief. You can say: “I’ve noticed you seem to be struggling. I care about you. Are you having thoughts of suicide?” If they say yes, take it seriously. Listen without judgment. Help them access support — whether that is calling 988 together, taking them to an emergency room, or contacting a mental health professional. Do not leave them alone if you believe they are in immediate danger. The 988 Lifeline also has resources specifically for people concerned about someone else.
Is this test a substitute for a professional evaluation?
No. This screening test cannot assess your personal risk level, determine the clinical severity of your ideation, or replace a comprehensive evaluation by a qualified mental health professional. What it can do is help you recognize the patterns present in your experience, understand the clinical framework used to assess suicidal ideation, and take a meaningful first step toward getting appropriate support. If your score is in the Moderate range or above — or if anything in the questions felt immediately and personally relevant — please reach out to a professional.
What treatments are available for suicidal ideation?
Suicidal ideation is treatable. Evidence-based approaches include Cognitive Behavioral Therapy (CBT), Dialectical Behavior Therapy (DBT — developed by Dr. Marsha Linehan specifically for high-risk populations, including individuals with chronic suicidal ideation), and Safety Planning Intervention (SPI). Research published in Frontiers in Psychiatry (2025) confirms that therapeutic approaches that strengthen reasons for living and protective factors produce significant reductions in suicidal ideation. Medication treatment for underlying conditions — particularly depression and bipolar disorder — also reduces suicidal ideation as a downstream effect. Recovery is possible. Help is available. The most important step is reaching out.
Related Tests
- Clinical Depression Test — depression is the most consistently documented risk factor for suicidal ideation; if depression is present alongside these thoughts, assess and address it directly
- Dysthymia Test — persistent low-grade depression that feels like personality rather than illness is associated with chronic suicidal ideation
- Anhedonia Test — loss of the capacity for pleasure is a core depression symptom strongly associated with suicidal ideation
- Bipolar Test — bipolar disorder is associated with significantly elevated suicidal ideation risk, particularly during depressive and mixed episodes
- Borderline Personality Disorder Test — BPD has among the highest rates of chronic suicidal ideation of any personality disorder
- Anxiety Test — anxiety disorders co-occur with suicidal ideation and both need to be assessed and addressed
- Burnout Test — severe burnout can produce hopelessness and passive suicidal ideation; worth screening for alongside depression
- High Functioning Depression Test — maintaining external function while experiencing severe internal distress is a pattern associated with concealed suicidal ideation
- PTSD Test — trauma history is a documented risk factor for suicidal ideation; PTSD and suicidal ideation frequently co-occur
For more mood and mental health assessments, visit our Mood and Depression collection.
References
- Posner, K., Brown, G.K., Stanley, B., et al. (2011). The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 168(12), 1266-1277. doi.org/10.1176/appi.ajp.2011.10111704
- Mundt, J.C., et al. (2013). Prediction of suicidal behavior using the Columbia Suicide Severity Rating Scale. Journal of Clinical Psychiatry. [Sensitivity 67%, specificity 76%] pmc.ncbi.nlm.nih.gov
- Harmer, B., Lee, S., Duong, T.V.H., & Saadabadi, A. (2024). Suicidal Ideation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. NBK565877. ncbi.nlm.nih.gov
- World Health Organization. (2023). Suicide. WHO Fact Sheet. who.int
- Centers for Disease Control and Prevention. (2024). Risk and Protective Factors for Suicide. cdc.gov
- CDC. (2023). Youth Risk Behavior Survey (YRBS) 2023. Mental Health and Suicide Risk Among High School Students. ncbi.nlm.nih.gov
- American Foundation for Suicide Prevention (AFSP). (2024). Ethical Reporting Guidelines for Media. [Safe messaging compliance] afsp.org
- Gómez-Tabares, A.S., et al. (2025). The Effect of Depression and Hopelessness on Suicidal Risk in Young People. Frontiers in Psychiatry. [14.56x risk interaction] pmc.ncbi.nlm.nih.gov
- Linehan, M.M., et al. Reasons for Living Inventory. [Protective factors framework] Referenced in Frontiers in Psychiatry, 2025. frontiersin.org
- 988 Suicide & Crisis Lifeline. (2024). 988lifeline.org
- International Association for Suicide Prevention (IASP). Crisis Centres Directory. iasp.info