
Most people who visit this page are not worried about themselves. They are here because of someone else — a parent who made everything about them, a partner whose warmth turned into contempt, a colleague whose confidence quietly became cruelty. They are here because something felt consistently, systematically wrong in a relationship, and they need language and a framework to understand it.
A smaller group comes here to question themselves. Perhaps someone close made a comment that landed differently, or certain relationship patterns keep repeating without a clear explanation. This kind of self-examination — especially for a condition as ego-syntonic as NPD — takes genuine courage.
This free Narcissistic Personality Disorder Quiz screens for both the grandiose and covert presentations of NPD using all nine DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Screens for the person in your life or for yourself. Instant, private results.
What Is Narcissistic Personality Disorder?
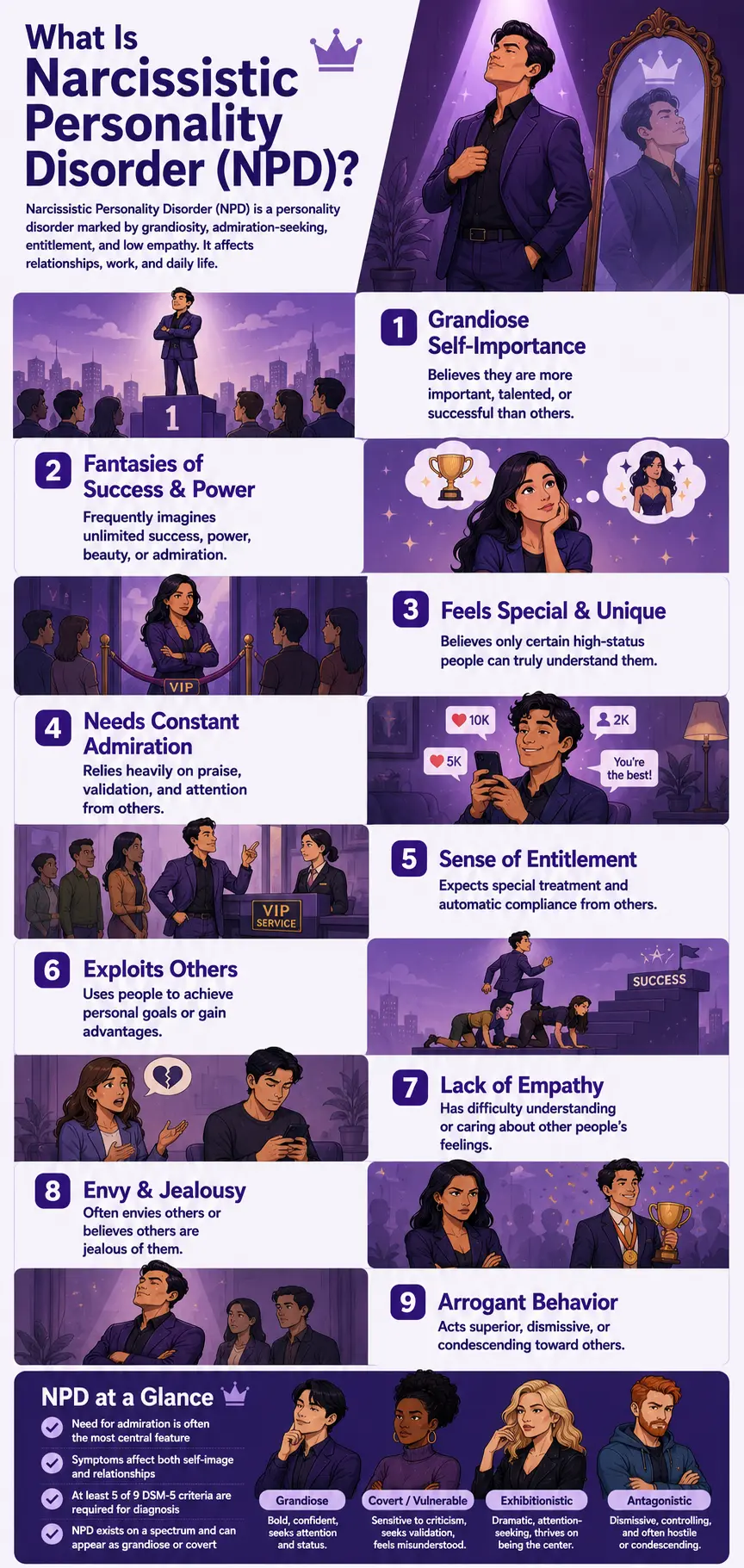
Narcissistic Personality Disorder (NPD) is a Cluster B personality disorder (DSM-5-TR code 301.81 / ICD-10: F60.81) — grouped alongside Borderline, Histrionic, and Antisocial Personality Disorders under the “dramatic, emotional, or erratic” cluster. The DSM-5-TR defines NPD as a pervasive pattern of grandiosity, need for admiration, and lack of empathy, beginning by early adulthood and present across multiple contexts (APA, 2022).
Prevalence estimates range from 0.5–5% of the general U.S. population (Rosenthal et al., 2020, cited in Frontiers in Behavioral Neuroscience, 2024), with clinical literature typically citing 1–2% (APA, 2022). Approximately 75% of those diagnosed are male — though the APA and researchers note this likely reflects diagnostic bias as much as genuine sex differences, since covert NPD is more common in women and is frequently misidentified or overlooked (APA, 2022).
A landmark 2025 network analysis of the DSM-5-TR NPD criteria, conducted by Gori and Topino (Clinical Psychology & Psychotherapy, 2025) with 376 mental health professionals, found that “need for admiration” emerged as the single most central node within the NPD criteria network — more clinically central than grandiosity itself. The analysis also identified two distinct symptom clusters in NPD: a self-dimension (grandiosity, fantasies, specialness, entitlement) and an interpersonal dimension (exploitation, empathy deficit, envy, arrogance). The central domain across both dimensions was antagonism — the shared disposition underlying all NPD expressions.
The DSM-5-TR diagnostic criteria for NPD — requiring at least 5 of the following 9 (APA, 2022):
- Criterion 1. A grandiose sense of self-importance — exaggerating achievements and talents, expecting to be recognized as superior without commensurate achievements.
- Criterion 2. Preoccupied with fantasies of unlimited success, power, brilliance, beauty, or ideal love.
- Criterion 3. Believes they are “special” and unique and can only be understood by, or should associate with, other high-status people or institutions.
- Criterion 4. Requires excessive admiration.
- Criterion 5. Has a sense of entitlement — unreasonable expectations of especially favorable treatment or automatic compliance.
- Criterion 6. Interpersonally exploitative — takes advantage of others to achieve their own ends.
- Criterion 7. Lacks empathy — unwilling to recognize or identify with the feelings and needs of others.
- Criterion 8. Often envious of others or believes that others are envious of them.
- Criterion 9. Shows arrogant, haughty behaviors or attitudes.
An important clinical note: the DSM-5-TR Section II criteria primarily describe the grandiose presentation of NPD. The APA’s own Section III Alternative Model of Personality Disorders recognizes that these criteria do not fully capture the vulnerable or covert subtype, which presents differently on the surface while sharing the same underlying dynamics (APA, 2022; Caligor, Levy & Clarkin, 2015).
Signs You Might Be Dealing With a Narcissist (Or Recognizing It in Yourself)
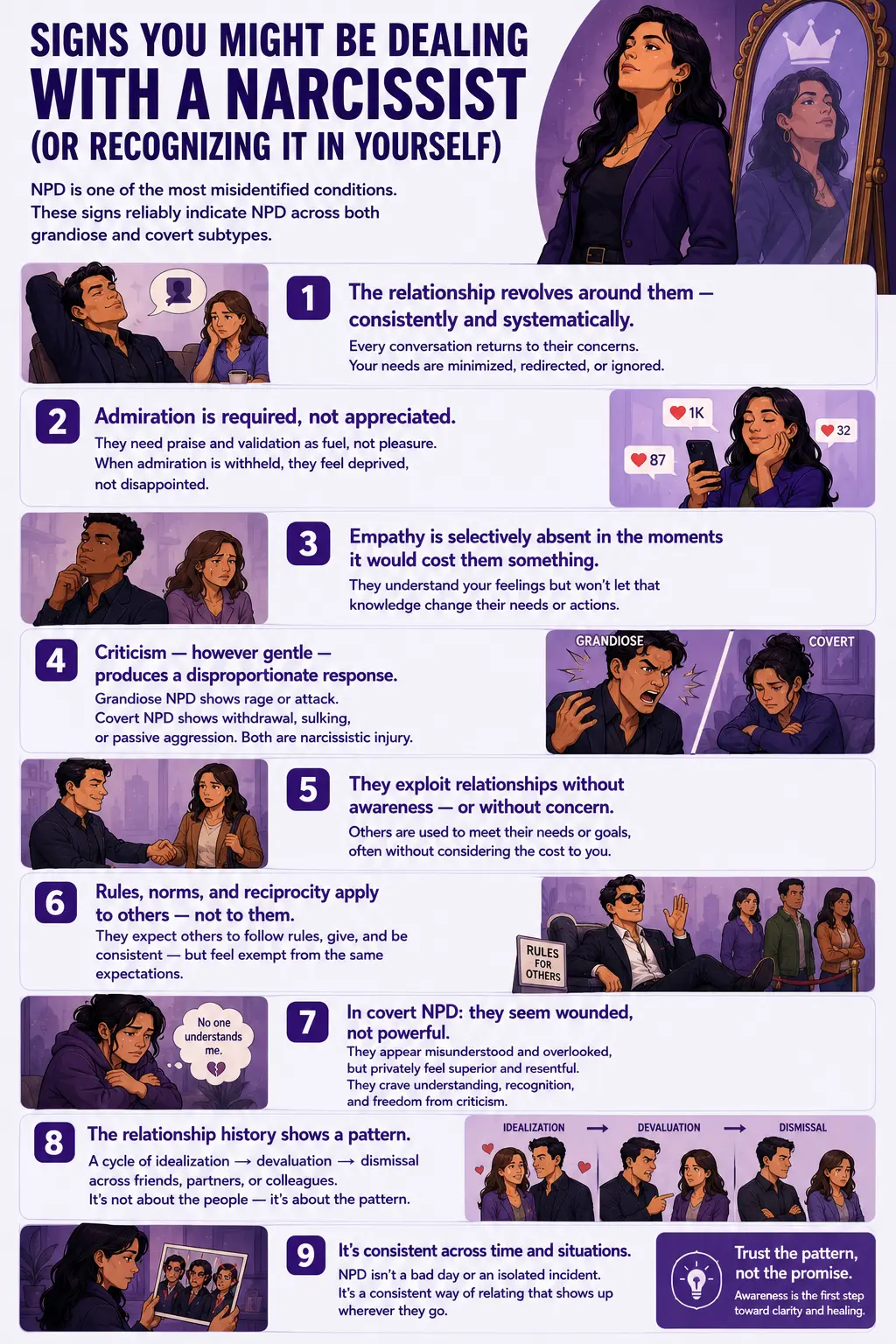
NPD is one of the most consistently misidentified conditions in psychology — because the grandiose version is obvious in retrospect but often compelling in the moment, and the covert version is almost invisible until you understand the pattern. These are the signs that most reliably indicate NPD, across both subtypes.
The relationship revolves around them — consistently and systematically. Not occasionally, as happens in any relationship when someone needs support. Consistently. Every significant conversation eventually returns to their concerns, their feelings, their narrative. Your needs, your experiences, and your emotional states are acknowledged briefly, if at all, and then redirected. Over time, you may find yourself editing your own experience before bringing it to them — anticipating that it won’t land, won’t matter, or will somehow circle back to being about them.
Admiration is required, not appreciated. Most people enjoy recognition and compliments. Someone with NPD requires them in a way that is qualitatively different — as fuel, not pleasure. When admiration is withheld or simply absent, the response is not disappointment but something more like deprivation. The need for admiration identified by Gori and Topino (2025) as the most central node in the NPD criteria network is not a preference — it is a structural requirement.
Empathy is selectively absent in the specific moments it would cost them something. People with NPD frequently can demonstrate knowledge of others’ emotional states — they can identify what someone is feeling. What they cannot consistently do is allow that knowledge to outweigh their own needs when the two conflict. The empathy deficit in NPD is not necessarily a failure to understand others’ emotions; it is a failure to let those emotions matter when it is inconvenient for them to do so.
Criticism — however gentle or well-intentioned — produces a disproportionate response. What the APA describes as “narcissistic injury” is the specific, intense response to perceived criticism, slights, or challenges to the self-image. In grandiose NPD, this looks like rage, contempt, or counterattack. In covert NPD, it looks like extended withdrawal, sulking, passive aggression, or a hurt silence that subtly communicates that you have done something wrong. Both are responses to the same underlying wound — a fragile self-esteem that the grandiosity exists to protect.
They exploit relationships without awareness — or without concern. Not all exploitation in NPD is calculated. Much of it is a simple absence of the consideration that most people apply automatically: “What does this cost the other person?” The exploitative behavior that characterizes NPD criterion 6 is often not malicious — it is the product of a fundamental orientation in which others exist primarily as extensions of one’s own needs and goals.
Rules, norms, and reciprocity apply to others — not to them. The entitlement in NPD (criterion 5) produces a specific orientation toward social rules: they apply to other people. Waiting in line, following social conventions, reciprocating favors, meeting commitments — these expectations apply to the people around them, not to them specifically, because their specialness exempts them from the ordinary obligations that govern everyone else.
In covert NPD specifically: they seem wounded, not powerful. The covert narcissist does not brag openly. Instead, they seem chronically misunderstood, perpetually overlooked, unfairly treated by a world that fails to recognize their special qualities. They are hypersensitive to perceived slights. They may appear shy, modest, or self-deprecating while privately feeling superior and resentful. Even gentle criticism can feel like an attack and may produce days of wounded withdrawal. The underlying grandiosity is present — it simply manifests as an entitlement to being understood, recognized, and never criticized, rather than as overt boastfulness.
The relationship history shows a pattern. NPD doesn’t produce isolated incidents — it produces a pattern across relationships and over time. Former friends, former partners, former colleagues who were initially close and then became targets of contempt or dismissal. A history of relationships that began with intense idealization and ended in devaluation. The pattern is not about specific circumstances — it is about the consistent dynamics that the person’s personality produces wherever they go.
Grandiose NPD vs Covert (Vulnerable) NPD — The Distinction That Changes Everything
This distinction is the most clinically important aspect of understanding NPD — particularly if you are here trying to make sense of someone in your life who doesn’t fit the obvious, boastful stereotype.
| Feature | Normal Narcissistic Traits | Grandiose (Overt) NPD | Covert (Vulnerable) NPD |
|---|---|---|---|
| External presentation | Confident, self-assured, sometimes self-focused | Openly boastful, obviously arrogant, dominant, attention-commanding | Quiet, withdrawn, apparently modest or even self-critical; may seem shy or sensitive |
| Grandiosity expression | Pride in genuine accomplishments; proportionate | Exaggerated, overt, actively promoted; expects recognition without commensurate achievement | Internal, hidden; “I am special and misunderstood” rather than “I am superior” — but the belief is the same |
| Response to criticism | Discomfort but proportionate adjustment | Narcissistic rage, contempt, counterattack, devaluation of the critic | Prolonged wounded withdrawal, sulking, passive aggression, shame spiral, hurt silence lasting days |
| Empathy | Genuine and consistent in most contexts | Absent when it conflicts with self-interest; can perform empathy when useful | Often appears emotionally sensitive; may show empathy in low-stakes contexts; absent when self-interest conflicts |
| Self-esteem structure | Stable and self-sustaining | Externally dependent — requires admiration and deference as ongoing fuel; fragile beneath the confidence | Overtly low or fragile; hypersensitive to any slight; same external dependency but through victimhood rather than dominance |
| Validated instrument | NPI (below threshold) | NPI (Raskin & Hall 1979); DSM-5-TR 9 criteria | MCNS (Cheek, Hendin & Wink 2013, alpha=.89); HSNS (Hendin & Cheek 1997) |
| Gender distribution | No significant pattern | More commonly diagnosed in males (APA DSM-5-TR 2022) | More common in females and significantly underdiagnosed (APA DSM-5-TR 2022) |
Both subtypes share the same core: an inflated self-importance, a fragile and externally-dependent self-esteem, an absence of genuine empathy when it costs something, and an enduring need for validation and admiration. The difference is entirely in how these features are expressed. As Caligor, Levy, and Clarkin (2015) document, individuals with NPD “may be grandiose or self-loathing, extraverted or socially isolated, captains of industry or unable to maintain steady employment” — all within the same diagnostic category.
Many people with NPD move between grandiose and vulnerable states depending on circumstance. Periods of success activate overt grandiosity; setbacks, losses, or perceived slights activate the covert, withdrawn, wounded presentation. Both states belong to the same person and reflect the same underlying structure.
The Maladaptive Covert Narcissism Scale (MCNS)
Given that the covert narcissism cluster represents the majority of searches arriving at this page — “covert narcissist quiz,” “maladaptive covert narcissism scale,” “vulnerable narcissist test,” “female covert narcissist test” — this section deserves specific attention.
The Maladaptive Covert Narcissism Scale (MCNS) was developed by Dr. Jonathan M. Cheek, Harvey M. Hendin, and Paul Wink at Wellesley College in 2013. It is a 23-item self-report instrument specifically designed to measure covert (vulnerable) narcissistic traits — the hypersensitive, shame-prone, socially withdrawn expression of narcissism that the standard DSM Section II criteria and the widely used Narcissistic Personality Inventory (NPI) consistently miss.
Key validation data: the MCNS has Cronbach alpha reliability of .89 (Cheek, Hendin & Wink, 2013, N=420, with replication in N=182 college women), significantly outperforming the earlier Hypersensitive Narcissism Scale (HSNS; alpha=.75). It correlates .65 with the MMPI composite measure of covert narcissism and shows strong construct validity across multiple samples (Cheek et al., 2013).
The MCNS specifically measures: need for external validation and admiration; high introversion; hypersensitivity to perceived criticism, humiliation, neglect, or belittlement; shame sensitivity; social withdrawal; emotional dysregulation; a tendency toward interpersonal conflict despite an apparently humble self-presentation; and a sense of persistent misrecognition — the feeling of being overlooked or undervalued by a world that doesn’t appreciate one’s special qualities (Cheek et al., 2013; Miller et al., 2012).
This Narcissistic Personality Disorder Quiz covers the covert narcissism dimension through the questions most relevant to the MCNS framework, alongside the grandiose criteria from the DSM-5-TR. The dedicated Covert Narcissism Test provides a more focused assessment of this specific profile.
What Causes Narcissistic Personality Disorder?
NPD develops from an interaction of developmental, relational, and possibly neurobiological factors. No single cause has been established, but several contributing pathways have consistent research support.
Developmental origins — two distinct pathways. Research and clinical observation have identified two distinct developmental pathways to NPD. In the first, the child receives excessive, unconditional praise and admiration disconnected from their actual behavior or achievements — creating an inflated self-concept that must be continuously maintained by external validation. In the second, the child experiences significant emotional neglect, humiliation, or criticism — developing grandiosity as a defensive structure against the profound shame and inadequacy beneath. Both pathways produce the same outcome: a self-concept that is both inflated and fragile, requiring continuous external reinforcement to sustain.
Parenting patterns. Research consistently links NPD with parenting styles characterized by either overvaluation (treating the child as special and exceptional regardless of behavior) or cold, neglectful parenting that fails to provide adequate mirroring and validation. The common thread is the failure to provide the kind of consistent, warm, reality-grounded validation that enables stable self-esteem to develop.
Neurobiological factors. Neuroimaging research has identified structural differences in areas associated with empathy, emotional regulation, and self-processing in individuals with NPD — including reduced grey matter volume in insular cortex regions associated with empathic processing (Schulze et al., 2013). These findings do not determine outcomes but suggest that biological vulnerability may interact with developmental experience in NPD etiology.
Comorbidities. NPD has high rates of comorbidity. The 2025 network analysis by Gori and Topino notes that NPD is associated with increased risk of comorbid mood disorders (Nagel et al., 2023), addictions, and other personality disorders. The Borderline Personality Disorder Test, Antisocial Personality Disorder Test, and Dark Triad Test are all worth completing where NPD is suspected, given documented overlap with these presentations.
How This Test Works
This Narcissistic Personality Disorder Quiz covers all nine DSM-5-TR criteria for NPD across 15 questions, weighted to capture both the grandiose and covert presentations. The questions assess grandiosity, need for admiration, entitlement, exploitation, empathy deficit, envy, arrogance, and the covert features of hypersensitivity and shame-based withdrawal.
The test can be completed for yourself or answered with someone else in mind — answering how they typically behave rather than how you do. Both uses are clinically valid and produce interpretable results.
Answer based on consistent patterns over the past 12 months — not isolated incidents or best/worst moments.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. This is a screening tool — only a qualified mental health professional can diagnose NPD through comprehensive clinical assessment.
Understanding Your NPD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few NPD Indicators | Few significant NPD patterns present. Normal self-confidence, occasional self-focus, or situational traits may be present without a pattern consistent with Narcissistic Personality Disorder. |
| 16 – 30 | Mild — Some Narcissistic Patterns | Some narcissistic patterns present across multiple domains. May not reach clinical NPD threshold, but patterns are meaningful and warrant reflection or professional discussion. |
| 31 – 45 | Moderate — Significant NPD Pattern | Significant narcissistic pattern across multiple criteria consistent with NPD. Professional evaluation is recommended — both for the person being described and for the person completing the test if it is self-directed. |
| 46 – 60 | High — Strong NPD Indicators | Pervasive and severe narcissistic pattern across most criteria. Professional evaluation is strongly recommended. |
NPD in the Cluster B Context
NPD does not exist in isolation. Understanding its relationship to the other Cluster B personality disorders is clinically important — both for accurate identification and for understanding what overlapping features mean.
Borderline Personality Disorder (BPD) shares emotional sensitivity, fear of rejection, and unstable relationships with NPD. The key distinction: BPD involves a visible, openly distressing vulnerability and fear of abandonment that NPD does not — the vulnerability in BPD is on the surface, while in NPD it is defended against by grandiosity. Both can involve intense reactions to perceived rejection, but the underlying structure differs fundamentally.
Antisocial Personality Disorder (ASPD) shares exploitative behavior and empathy deficit with NPD. The distinction: ASPD involves a more pervasive and consistent disregard for rules and others’ rights, often with a history of conduct problems in childhood. NPD’s exploitation is typically more status-oriented and less consistently predatory than ASPD’s. Both can co-occur.
Dark Triad traits — narcissism, Machiavellianism, and psychopathy — all correlate with NPD at the subclinical level. High Dark Triad scores, particularly on the narcissism dimension, may indicate clinically significant NPD patterns worth formal evaluation.
Frequently Asked Questions
What is Narcissistic Personality Disorder?
Narcissistic Personality Disorder (NPD) is a Cluster B personality disorder (DSM-5-TR 301.81 / F60.81) defined as a pervasive pattern of grandiosity, need for admiration, and lack of empathy, beginning by early adulthood and present across multiple contexts. Diagnosis requires at least 5 of 9 DSM-5-TR criteria. Prevalence is estimated at 0.5–5% of the general population, with approximately 75% of diagnoses in males — though this reflects diagnostic bias as much as real sex differences, since covert NPD is more prevalent in women and significantly underdiagnosed (APA, 2022; Frontiers in Behavioral Neuroscience, 2024). A 2025 network analysis (Gori & Topino) identified “need for admiration” as the most central node in the NPD criteria network, with antagonism as the central personality domain.
What is the difference between grandiose and covert narcissism?
Grandiose (overt) NPD is the obvious, externally visible form — openly boastful, dominant, contemptuous, and attention-commanding. Covert (vulnerable) NPD presents very differently on the surface: quiet, apparently modest or self-critical, chronically misunderstood, hypersensitive to criticism, prone to withdrawal and hurt silence. Both subtypes share the same core — inflated self-importance, fragile, externally dependent self-esteem, an empathy deficit, and a persistent need for validation. The difference is in expression, not in the underlying structure. Covert NPD is specifically measured by the Maladaptive Covert Narcissism Scale (MCNS; Cheek, Hendin & Wink, 2013, alpha=.89).
Can someone with NPD change?
Change is possible but requires the person to recognize and be troubled by the pattern — which is the primary obstacle, since NPD is ego-syntonic (experienced as correct rather than problematic). Schema Therapy and Transference-Focused Psychotherapy (TFP) have the strongest evidence base for NPD treatment. Both address the underlying developmental schemas and self-structure driving the narcissistic pattern. The prognosis depends significantly on the person’s capacity for genuine self-reflection and their motivation to change based on what the patterns are actually costing them — in relationships, in their sense of meaning, and in their own wellbeing.
Is NPD more common in men or women?
Approximately 75% of NPD diagnoses are male (APA, 2022). However, researchers and the APA itself note this likely reflects diagnostic bias as much as genuine sex differences — the DSM-5-TR Section II criteria primarily describe the grandiose presentation, which is more stereotypically male. Covert (vulnerable) NPD, which is more common in women, is frequently misidentified, unrecognized, or diagnosed as another condition (depression, anxiety, BPD). The actual sex ratio for NPD, if both presentations were equally well-recognized, is believed to be closer to equal (APA, 2022).
How is NPD different from healthy confidence or high self-esteem?
Healthy confidence is stable, self-sustaining, and does not require continuous external validation to maintain. It can tolerate criticism without producing rage or withdrawal. It includes genuine empathy that is available even when it is inconvenient. NPD is characterized by the opposite of stability: a self-concept that is both inflated and fragile, requiring constant admiration as fuel, collapsing into shame or rage when challenged, and unable to sustain genuine empathy when it conflicts with self-interest. The surface behavior may look like confidence, but the internal structure is fundamentally insecure. As the APA notes, those with NPD “may be very sensitive to criticism or defeat, and although they may not show it, those experiences may leave them feeling ashamed, degraded, and empty” (APA, 2022).
Can I be in a relationship with someone with NPD?
Yes — many people are, often for years before the pattern is recognized for what it is. Whether to stay in that relationship depends on many factors specific to your situation, including the severity of the NPD, whether the person is in treatment, and the impact on your own well-being. What the research and clinical experience consistently show is that you cannot change the person with NPD through love, patience, accommodation, or trying harder. What you can do is access support for yourself — through therapy that helps you understand the dynamics, establish protective boundaries, and make informed choices about the relationship. The most important step for anyone in a relationship with a high-NPD person is getting appropriate professional support for themselves.
What is the Maladaptive Covert Narcissism Scale (MCNS)?
The Maladaptive Covert Narcissism Scale (MCNS) is a 23-item self-report instrument developed by Cheek, Hendin, and Wink (2013) at Wellesley College to measure covert (vulnerable) narcissistic traits. Unlike the standard NPI (which measures grandiose narcissism), the MCNS specifically captures the hypersensitive, shame-prone, withdrawn expression of narcissism. It has a Cronbach alpha reliability of .89 and correlates .65 with the MMPI measure of covert narcissism. The Covert Narcissism Test provides a dedicated assessment based on the MCNS framework.
Related Tests
- Covert Narcissism Test — dedicated assessment for vulnerable/covert NPD using the MCNS framework; most relevant for the quiet, sensitive, misunderstood presentation
- Dark Triad Test — narcissism as one of three dark personality dimensions; useful for understanding the broader trait context
- Borderline Personality Disorder Test — BPD and NPD overlap in emotional sensitivity and unstable relationships; important to distinguish
- Antisocial Personality Disorder Test — shares exploitative behavior and empathy deficit with NPD; both are Cluster B
- Psychopath Test (PCL-R) — psychopathy and NPD overlap in callousness and entitlement; distinct in other features
- Empathy Test — reduced empathy is the most diagnostically specific NPD feature; complementary assessment
- Histrionic Personality Disorder Test — both are Cluster B; HPD and NPD share attention-seeking and dramatic behavior patterns
- Anxiety Test — NPD is associated with elevated comorbid anxiety; the shame-prone covert presentation in particular
- Clinical Depression Test — comorbid mood disorders are well-documented in NPD (Nagel et al. 2023)
- Full Personality Disorder Test Hub — all ten DSM-5-TR personality disorder types
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Narcissistic Personality Disorder 301.81 (F60.81), pp. 760–764. psychiatry.org
- Gori, A., & Topino, E. (2025). DSM-5-TR Criteria and Domains for Narcissistic Personality Disorder: Evidence From Network Analysis Based on the Mental Health Professionals’ Perspective. Clinical Psychology & Psychotherapy, 32(6), e70179. [Need for admiration = most central node; N=376] doi.org/10.1002/cpp.70179
- Cheek, J.M., Hendin, H.M., & Wink, P. (2013). An Expanded Version of the Hypersensitive Narcissism Scale: The Maladaptive Covert Narcissism Scale. [MCNS; alpha=.89; N=420+182] academia.edu
- Rosenthal, S.A., et al. (2020). Narcissistic Personality Disorder. In: Encyclopedia of Personality and Individual Differences. [0.5–5% prevalence] Cited in Frontiers in Behavioral Neuroscience (2024). doi.org/10.3389/fnbeh.2024.1354258
- Caligor, E., Levy, K.N., & Clarkin, J.F. (2015). Narcissistic Personality Disorder: Diagnostic and Clinical Challenges. American Journal of Psychiatry, 172(5), 415–422. doi.org/10.1176/appi.ajp.2014.14060723
- Miller, J.D., et al. (2012). Grandiose and Vulnerable Narcissism: A Nomological Network Analysis. Journal of Personality, 79(5), 1013–1042. [Vulnerable narcissism: higher anxiety + lower self-esteem] doi.org
- Hendin, H.M., & Cheek, J.M. (1997). Assessing hypersensitive narcissism: A reexamination of Murray’s Narcism Scale. Journal of Research in Personality, 31, 588–599. [HSNS — predecessor to MCNS]
- Schulze, L., et al. (2013). Gray matter abnormalities in patients with narcissistic personality disorder. Journal of Psychiatric Research, 47(10), 1363–1369. doi.org
- Ronningstam, E. (2011). Narcissistic personality disorder in DSM-V — In support of retaining a significant diagnosis. Journal of Personality Disorders, 25(2), 248–259. doi.org
- Wikipedia. (2025). Narcissistic personality disorder. en.wikipedia.org