Not everyone who doubts people’s motives has Paranoid Personality Disorder. Caution is reasonable. Healthy skepticism is adaptive. But there is a threshold — a point where mistrust becomes pervasive, where it operates regardless of evidence, where it shapes every relationship and every interaction, where it becomes impossible to trust even the people closest to you for sustained periods of time.
That threshold is what Paranoid Personality Disorder (PPD) describes. Not occasional suspicion — a chronic, deeply ingrained pattern of interpreting others’ intentions as malevolent, beginning in early adulthood and present across a wide variety of contexts. It is one of the most commonly occurring personality disorders, affecting an estimated 2.3–4.4% of the general population, and among the most frequently missed, because people with PPD rarely self-identify as paranoid. They experience themselves as appropriately vigilant in a world that genuinely cannot be trusted.
This free Paranoid Personality Disorder test screens for the patterns associated with Paranoid Personality Disorder using all seven DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Based on your experience over the past 12 months. Results are instant and private.
What Is Paranoid Personality Disorder?
Paranoid Personality Disorder (PPD) is a Cluster A personality disorder — grouped alongside Schizoid Personality Disorder and Schizotypal Personality Disorder under the DSM-5-TR’s “odd or eccentric” cluster. Its defining feature is a pervasive, persistent pattern of distrust and suspiciousness toward others — interpreting their motives as malevolent — that begins in early adulthood and is present across multiple contexts.
The DSM-5-TR (APA, 2022) classifies PPD under code 301.0 (ICD-10: F60.0). For a diagnosis, the pervasive distrust must be evidenced by at least four of the following seven criteria:
- Unjustified suspicion of exploitation or harm. Suspects, without sufficient basis, that others are exploiting, harming, or deceiving them — interpreting interactions through a lens of potential threat even when no objective evidence supports this.
- Preoccupation with unjustified doubts about loyalty. Preoccupied with doubts about the loyalty or trustworthiness of friends, colleagues, or family members — even those with established relationships. Small inconsistencies become evidence of larger betrayals.
- Reluctance to confide due to fear of exploitation. Reluctant to share personal information, disclose vulnerabilities, or confide in others out of fear that the information will be used maliciously against them.
- Reading hidden meanings into benign remarks or events. Reads demeaning, hostile, or threatening subtext into ordinary remarks, looks, or events that others interpret as neutral. A casual comment becomes an attack; an innocent question becomes an interrogation.
- Persistent grudge-bearing. Bears grudges — are unforgiving of perceived insults, injuries, or slights, often indefinitely. Minor offenses are not forgiven or forgotten; they are cataloged and remain emotionally live long after the event.
- Perceiving character attacks and counterattacking rapidly. Perceives attacks on their character or reputation that are not apparent to others, and responds quickly with anger or counterattack. Hypersensitivity to criticism combined with rapid defensive escalation.
- Recurrent suspicions about the fidelity of a partner. Has recurrent, unjustified suspicions regarding the sexual or romantic fidelity of their partner, without sufficient cause, and is resistant to reassurance.
These patterns must be stable and pervasive, not better explained by another psychotic or mood disorder, and must cause clinically significant distress or functional impairment (APA, 2022).

What Paranoid Personality Disorder Actually Feels Like
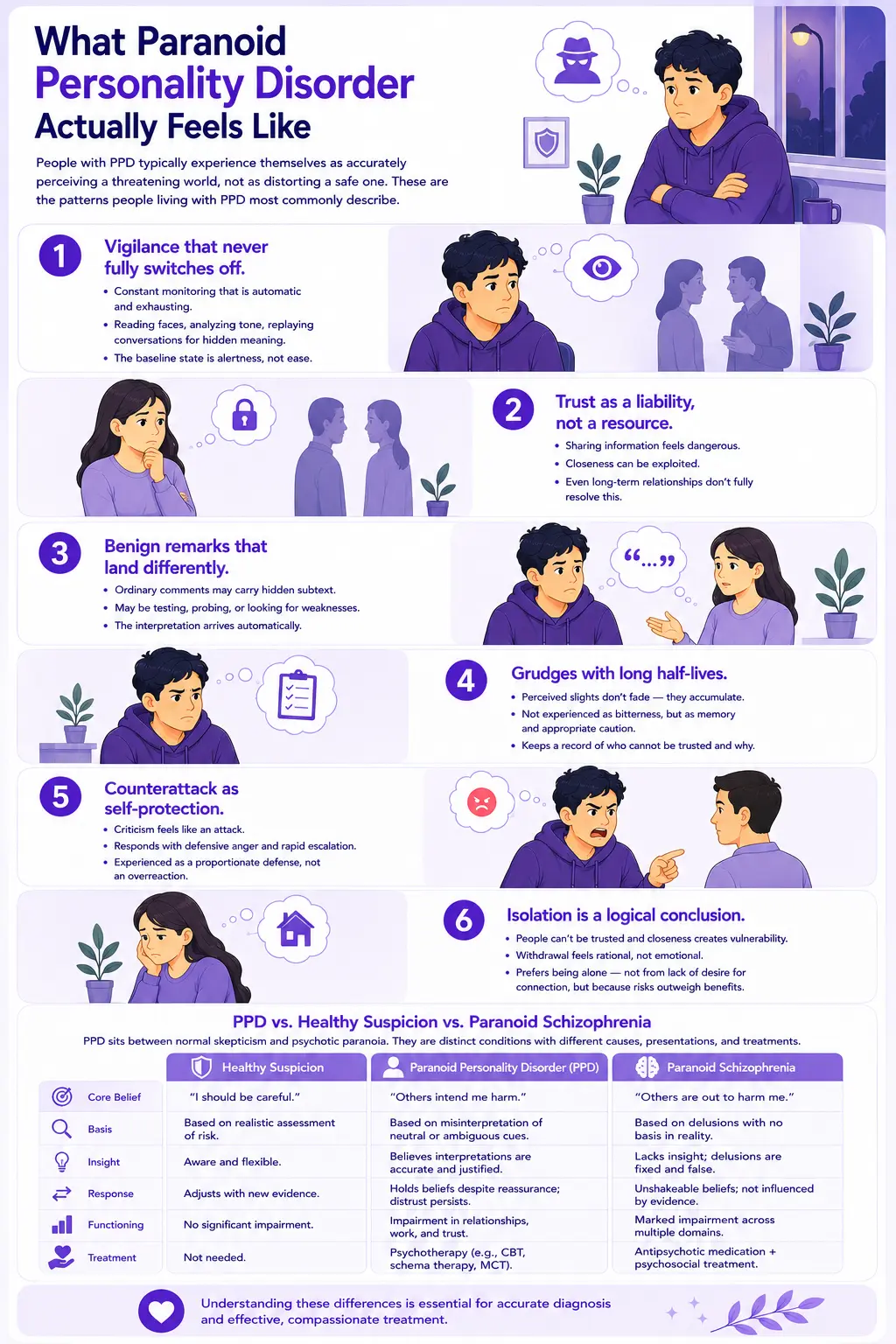
Because PPD is rarely self-reported as paranoia — people with the disorder typically experience themselves as accurately perceiving a threatening world, not as distorting a safe one — it is important to describe what the disorder looks like from the inside. These are the patterns people living with PPD most commonly describe:
- Vigilance that never fully switches off. Social situations require constant monitoring — not consciously chosen, but automatic and exhausting. Reading faces for microexpressions of contempt. Analyzing tone of voice for signs of condescension. Replaying conversations for evidence of hidden meaning. The baseline state is alertness, not ease.
- Trust as a liability, not a resource. Sharing personal information feels dangerous. Confiding creates a vulnerability that could be exploited. Closeness is something others want from you for their own reasons — not something that can be safely offered in both directions. Even long-term relationships do not fully resolve this.
- Benign remarks that land differently. A colleague’s offhand comment, a partner’s casual question, a friend’s joke — these are not neutral. They carry subtext. They may be testing you, probing for weaknesses, looking for something to use. The interpretation is not chosen — it arrives automatically, before any other reading is possible.
- Grudges with long half-lives. Perceived slights do not fade. They accumulate into a comprehensive record of who cannot be trusted and why. This is not experienced as bitterness — it is experienced as memory, as appropriate caution about demonstrated patterns of behavior.
- Counterattack as self-protection. When criticized, the response is not hurt — it is defensive anger, rapid escalation, a readiness to reframe the criticism as an attack and respond accordingly. This is not experienced as an overreaction but as a proportionate defense against unjustified aggression.
- Isolation is a logical conclusion. Given that people cannot be trusted and that closeness creates vulnerability, withdrawal is the rational response. Many people with PPD describe preferring to be alone — not because they don’t want connection, but because the risks of connection feel consistently greater than the benefits.
- PPD vs. Healthy Suspicion vs. Paranoid Schizophrenia
One of the most clinically important questions around PPD is distinguishing it from normal skepticism on one end and psychotic paranoia on the other. These are genuinely distinct conditions with different etiologies, presentations, and treatments.
| Feature | Healthy Suspicion | Paranoid Personality Disorder | Paranoid Schizophrenia / Psychosis |
|---|---|---|---|
| Reality testing | Intact — can update beliefs based on evidence | Intact — no delusions or hallucinations; beliefs are overvalued, not delusional | Impaired — delusions and/or hallucinations present; beliefs may be clearly false |
| Relationship to evidence | Responsive to evidence; suspicion reduces when contradicted | Evidence-resistant; contrary evidence may reinforce rather than reduce suspicion | Delusional — belief maintained despite clear evidence to the contrary |
| Onset and duration | Situationally triggered; resolves | Pervasive and chronic — begins in early adulthood, present across all contexts | Often episodic — may have periods of relative remission; often more acute onset |
| Hallucinations | Absent | Absent (by definition — if present, reclassify) | Often present — auditory hallucinations are the most common |
| Insight | Fully aware when being suspicious | Limited — typically does not recognize beliefs as distorted; experiences them as realistic | Often absent, a person may have no awareness of illness |
| Functional impact | Minimal | Significant — relationships, work, and daily life are chronically impaired | Severe — often acutely impairing; may require hospitalization |
| PsyMed screening | No screening needed | This test | Schizotypal Test as a starting point |
This distinction matters because treatment differs significantly. PPD is treated with psychotherapy; antipsychotics, when used, are adjunctive rather than primary. Schizophrenia requires antipsychotic medication as the cornerstone of treatment. Misidentifying one as the other leads to inappropriate treatment approaches.
What Causes Paranoid Personality Disorder?
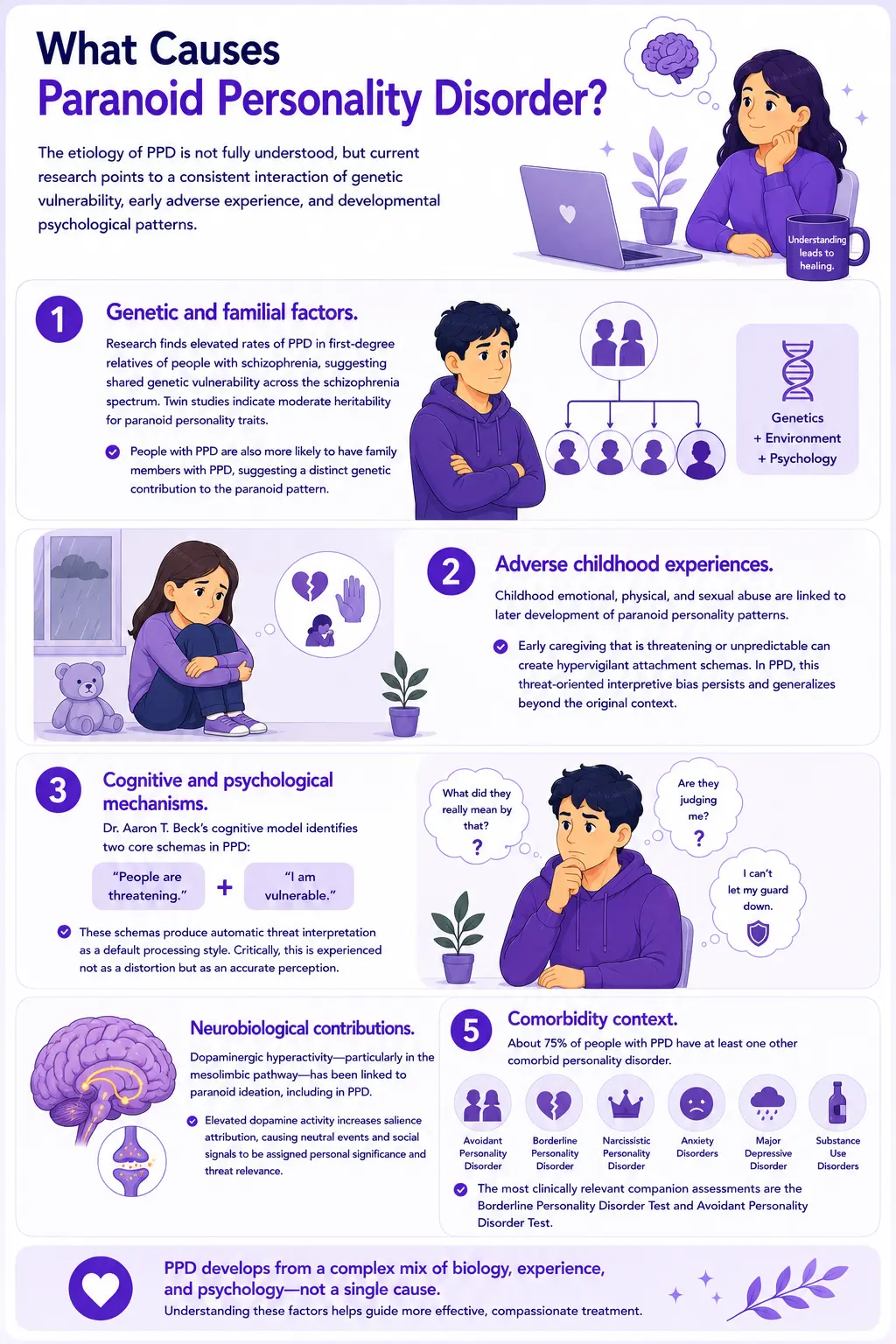
The etiology of PPD is not fully understood, but current research points to a consistent interaction of genetic vulnerability, early adverse experience, and developmental psychological patterns.
- Genetic and familial factors. PPD involves complex origins, including genetic, environmental, and psychological factors. Research finds elevated rates of PPD in first-degree relatives of people with schizophrenia, suggesting shared genetic vulnerability across the schizophrenia spectrum. Twin studies indicate moderate heritability for paranoid personality traits. People with PPD are also more likely to have family members with PPD specifically, suggesting a distinct genetic contribution to the paranoid pattern rather than purely schizophrenia spectrum genes.
- Adverse childhood experiences. Adverse childhood experiences are known to be a risk factor for PPD. Specifically, research links childhood emotional, physical, and sexual abuse with later development of paranoid personality patterns — a finding that has been replicated across multiple studies. The mechanism appears to involve the formation of hypervigilant attachment schemas: when early caregiving environments are genuinely threatening or unpredictable, a threat-oriented interpretive bias becomes adaptive. In PPD, this bias persists and generalizes beyond the original threatening context.
- Cognitive and psychological mechanisms. Dr. Aaron T. Beck’s cognitive model identifies specific information-processing patterns in PPD: a primary schema of “people are threatening” combined with a self-schema of “I am vulnerable” — producing automatic threat interpretation as a default processing style. Critically, this is experienced not as a distortion but as an accurate perception. The person with PPD is not aware of biasing their interpretations — they believe they are seeing clearly what others choose not to acknowledge.
- Neurobiological contributions. Research on dopaminergic hyperactivity — particularly in the mesolimbic pathway — has implicated dopamine dysregulation in paranoid ideation more broadly, including PPD. Elevated dopaminergic activity produces heightened salience attribution: events and social signals are assigned personal significance and threat relevance that they would not have under normal dopamine tone.
- Comorbidity context. It is estimated that 75% of people with PPD also have another comorbid personality disorder, with the most common ones being avoidant and borderline personality disorders, followed by narcissistic personality disorder. Anxiety disorders, major depressive disorder, and substance use disorders are also commonly comorbid. The Borderline Personality Disorder Test and Avoidant Personality Disorder Test are the most clinically relevant companion assessments.
How This PPD Test Works
This test screens for Paranoid Personality Disorder using the seven DSM-5-TR diagnostic criteria for PPD (APA, 2022) plus functional impact and duration domains — 15 questions total. The test is designed to capture the pervasive, chronic nature of PPD rather than acute situational reactions.
Answer based on your consistent, typical experience over the past 12 months — not your best periods, and not your worst episodes. The question is whether this pattern is your baseline, not whether you have ever experienced these things.
Never = 0 | Rarely = 1 | Sometimes = 2 | Often = 3 | Always = 4
Total range: 0–60. This is a screening tool — it cannot diagnose PPD. A significant score is clinically meaningful and worth discussing with a qualified mental health professional.
Understanding Your PPD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few PPD Indicators | Responses suggest a few significant paranoid personality patterns. Normal caution and occasional mistrust may be present without a pattern consistent with PPD. |
| 16 – 30 | Mild — Some Paranoid Patterns Present | Some paranoid personality patterns are present across at least some domains. May not reach the full PPD threshold, but is worth monitoring and discussing with a professional. |
| 31 – 45 | Moderate — Significant PPD Pattern | A significant pattern of paranoid personality symptoms is present across multiple domains. Consistent with PPD and warrants professional evaluation. |
| 46 – 60 | High — Strong PPD Indicators | Pervasive and severe paranoid personality patterns across most domains. Professional evaluation and support are strongly recommended. |
Treatment for Paranoid Personality Disorder — What the Evidence Shows
PPD is among the more challenging personality disorders to treat, primarily because the core feature of the disorder — difficulty trusting others — makes it difficult to establish the therapeutic relationship that treatment depends on. People with PPD may be suspicious of therapists’ motives, resistant to reframing their interpretations as distorted, and prone to premature treatment termination. These are not failures of motivation — they are features of the disorder that require specific clinical management.
- Cognitive Behavioral Therapy (CBT). The most studied and most commonly used approach for PPD. CBT targets the automatic threat-interpretation processes and the underlying core beliefs about others’ malevolence and one’s own vulnerability. Specific techniques include examining evidence for and against threat interpretations, conducting behavioral experiments that test predictions about others’ intentions, and investigating the cognitive schemas that maintain the paranoid interpretive bias. The challenge is that CBT requires a degree of collaborative trust in the therapeutic relationship that PPD makes difficult, which makes alliance-building the primary early clinical task.
- Schema Therapy. Addresses the early maladaptive schemas underlying PPD — particularly the “mistrust/abuse” schema that typically has roots in early adverse experience. Schema Therapy combines cognitive, behavioral, and experiential techniques with a specific focus on early developmental origins, making it particularly relevant for PPD, where childhood adversity is often a significant contributing factor.
- Metacognitive Training (MCT). A newer approach specifically targeting the metacognitive beliefs that maintain paranoid ideation — beliefs about the value of worry, the reliability of intuition about threat, and the importance of monitoring others for danger signs. MCT has emerging evidence across paranoia presentations and is increasingly being adapted for personality disorder contexts.
- Pharmacotherapy. No medications are specifically approved for PPD. Antipsychotic medications (low-dose) are sometimes used adjunctively for anxiety, agitation, or when paranoid ideation becomes particularly acute. SSRIs may be used for comorbid anxiety or depression. Medication does not address the core personality patterns but can reduce the intensity of symptoms enough to make psychotherapy more accessible.
- Treatment prognosis. With treatment, meaningful improvement in paranoid patterns and interpersonal functioning is achievable, though complete remission is less common than for Axis I conditions. Research suggests that the prognosis is better when treatment is initiated earlier, comorbidities are addressed, and a stable therapeutic alliance is established. The long-term goal is not the elimination of caution but the development of a more flexible and evidence-responsive relationship with trust.

Frequently Asked Questions
What is Paranoid Personality Disorder?
Paranoid Personality Disorder (PPD) is a Cluster A personality disorder defined by a pervasive, persistent pattern of distrust and suspiciousness of others, beginning by early adulthood and present across multiple contexts. The DSM-5-TR (301.0 / F60.0) requires the presence of at least 4 of 7 specific criteria, including unjustified suspicion of exploitation, preoccupation with doubts about loyalty, reluctance to confide, reading threatening meaning into benign events, persistent grudge-bearing, rapid counterattack when criticized, and unjustified jealousy in relationships. It affects approximately 2.3–4.4% of the general population and is more common in men.
What is the difference between PPD and being generally suspicious?
The key distinguishing features are pervasiveness, evidence-resistance, chronicity, and functional impact. Healthy suspicion is situation-specific, responsive to evidence, and resolves when circumstances change. PPD is present across all contexts, regardless of evidence — small inconsistencies are interpreted as confirming a pre-existing threat narrative rather than updating it. It begins by early adulthood, persists over the years, and causes clinically significant impairment in relationships and functioning. The person with PPD is not choosing to distrust — the threat interpretation arrives automatically and feels like an accurate perception.
Is paranoid personality disorder the same as paranoid schizophrenia?
No — these are distinct conditions. PPD is a personality disorder characterized by overvalued ideas about others’ malevolence. Reality testing is intact — there are no delusions or hallucinations. Paranoid schizophrenia involves frank psychosis: hallucinations (most commonly auditory), delusions (fixed false beliefs), and significant reality testing impairment. PPD is treated primarily with psychotherapy; schizophrenia requires antipsychotic medication as the cornerstone of treatment. The conditions can co-occur — PPD can be a premorbid condition that precedes a later schizophrenia diagnosis in some cases.
Can paranoid personality disorder be treated?
Yes, though it is among the more challenging personality disorders to treat because the core feature (distrust of others) makes it difficult to establish the therapeutic alliance that treatment requires. Cognitive Behavioral Therapy (CBT), Schema Therapy, and Metacognitive Training (MCT) all have evidence to support them. Meaningful improvement in paranoid patterns and interpersonal functioning is achievable with treatment, though the process typically requires a longer duration than for episodic conditions. Earlier intervention produces better outcomes. The primary barrier to treatment is that people with PPD often do not seek help — they experience themselves as correctly perceiving a threatening world rather than as experiencing a treatable disorder.
What are the signs of paranoid personality disorder?
The core signs are: persistent distrust and suspiciousness of others’ motives without sufficient basis; preoccupation with doubts about others’ loyalty; reluctance to confide out of fear of exploitation; reading hidden demeaning or threatening meanings into benign remarks; bearing grudges persistently; perceiving attacks on character and counterattacking rapidly; and recurrent unjustified suspicions about a partner’s fidelity. Functionally, these patterns produce chronic difficulty in close relationships, social isolation, occupational conflict, and a persistent background state of vigilance and suspicion. The person is typically unaware that these patterns are problematic — they experience them as realistic responses to an untrustworthy world.
Is paranoid personality disorder related to anxiety?
There is significant overlap and frequent comorbidity. Social anxiety disorder and PPD both involve vigilance in social situations and sensitivity to others’ evaluations — but the underlying driver differs. In social anxiety, the feared outcome is humiliation or negative evaluation; the person typically does not attribute hostile intent to others. In PPD, the core attribution is malevolence — others cannot be trusted because their intentions may be harmful. Both conditions frequently co-occur, and anxiety disorders are among the most common comorbidities in PPD. The Anxiety Test is worth completing if significant anxiety is present alongside these patterns.
What triggers paranoid personality disorder episodes?
PPD is not episodic in the way mood disorders are — it is a persistent personality pattern rather than a condition that waxes and wanes. However, certain situations reliably intensify paranoid patterns: high-stress environments, major life transitions, situations involving genuine uncertainty about others’ intentions, close relationships that require increasing vulnerability, and experiences that resemble earlier adverse experiences. Sleep deprivation, substance use (particularly stimulants and cannabis), and physical illness can also temporarily intensify paranoid patterns. Treatment focuses not on eliminating these intensifications but on building a more flexible interpretive repertoire that can accommodate ambiguity without defaulting to a threat response.
Related Tests
PPD rarely exists in isolation. These are the most clinically relevant companion assessments:
- Schizoid Personality Disorder Test — the other Cluster A disorder involving social detachment; important to distinguish as the underlying driver differs significantly from PPD
- Schizotypal Personality Disorder Test — Cluster A; shares some paranoid features but adds magical thinking and perceptual distortions; frequently comorbid with PPD
- Borderline Personality Disorder Test — one of the most common PPD comorbidities; shares fear of betrayal and interpersonal instability, but has different emotional and impulsivity features
- Narcissistic Personality Disorder Quiz — frequently comorbid; the hypersensitivity to criticism and rapid counterattack in PPD overlaps with narcissistic injury patterns
- Avoidant Personality Disorder Test — among the most common PPD comorbidities; shares social withdrawal but is driven by fear of rejection rather than distrust of motives
- Anxiety Test — anxiety disorders are among the most common PPD comorbidities; the vigilance and social sensitivity in both conditions frequently co-occur
- PTSD Test — childhood adversity and trauma are major PPD risk factors; PTSD and PPD frequently co-occur and can be clinically difficult to distinguish
- Attachment Style Test — paranoid personality patterns are strongly associated with disorganized or fearful-avoidant attachment; understanding attachment patterns can illuminate PPD origins
- Full Personality Disorder Test Hub — explore all ten DSM-5 personality disorder types across Clusters A, B, and C
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Paranoid Personality Disorder 301.0 (F60.0), pp. 737–741. psychiatry.org
- Jain, L., & Torrico, T.J. (2024). Paranoid Personality Disorder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Updated June 5, 2024. ncbi.nlm.nih.gov
- Merck Manual Professional Edition. (2025). Paranoid Personality Disorder (PPD). merckmanuals.com
- Triebwasser, J., Chemerinski, E., Roussos, P., & Siever, L.J. (2013). Paranoid personality disorder. Journal of Personality Disorders, 27(6), 795–805. pubmed.ncbi.nlm.nih.gov
- PsychDB. (2024). Paranoid Personality Disorder. psychdb.com
- Beck, A.T., Freeman, A., & Associates. (1990). Cognitive Therapy of Personality Disorders. Guilford Press.
- Grant, B.F., Hasin, D.S., Stinson, F.S., et al. (2004). Prevalence, correlates, and disability of personality disorders in the United States. Journal of Clinical Psychiatry, 65(7), 948–958.
- Wikipedia contributors. (2025). Paranoid personality disorder. Wikipedia, The Free Encyclopedia. en.wikipedia.org