
Plenty of people prefer their own company. Introversion, a love of solitude, needing time alone to recharge — none of these is a disorder, and most quiet, private people are perfectly healthy. Schizoid Personality Disorder is something distinct and much rarer: a deep, pervasive, lifelong pattern of detachment from social relationships combined with a genuinely limited range of emotional expression. The key difference is desire. People with social anxiety or avoidant personality avoid closeness because they fear rejection — they often want connection but find it too painful to pursue. The person with Schizoid Personality Disorder largely doesn’t desire closeness in the first place. Solitude isn’t a refuge from fear; it’s simply preferred.
This free Schizoid Personality Disorder Test screens for the traits of SPD using the DSM-5-TR diagnostic criteria (APA, 2022). 16 questions. Instant, private results. Like all such tools, it’s a starting point for reflection and not a diagnosis — only a qualified professional can diagnose a personality disorder.
What Is Schizoid Personality Disorder?
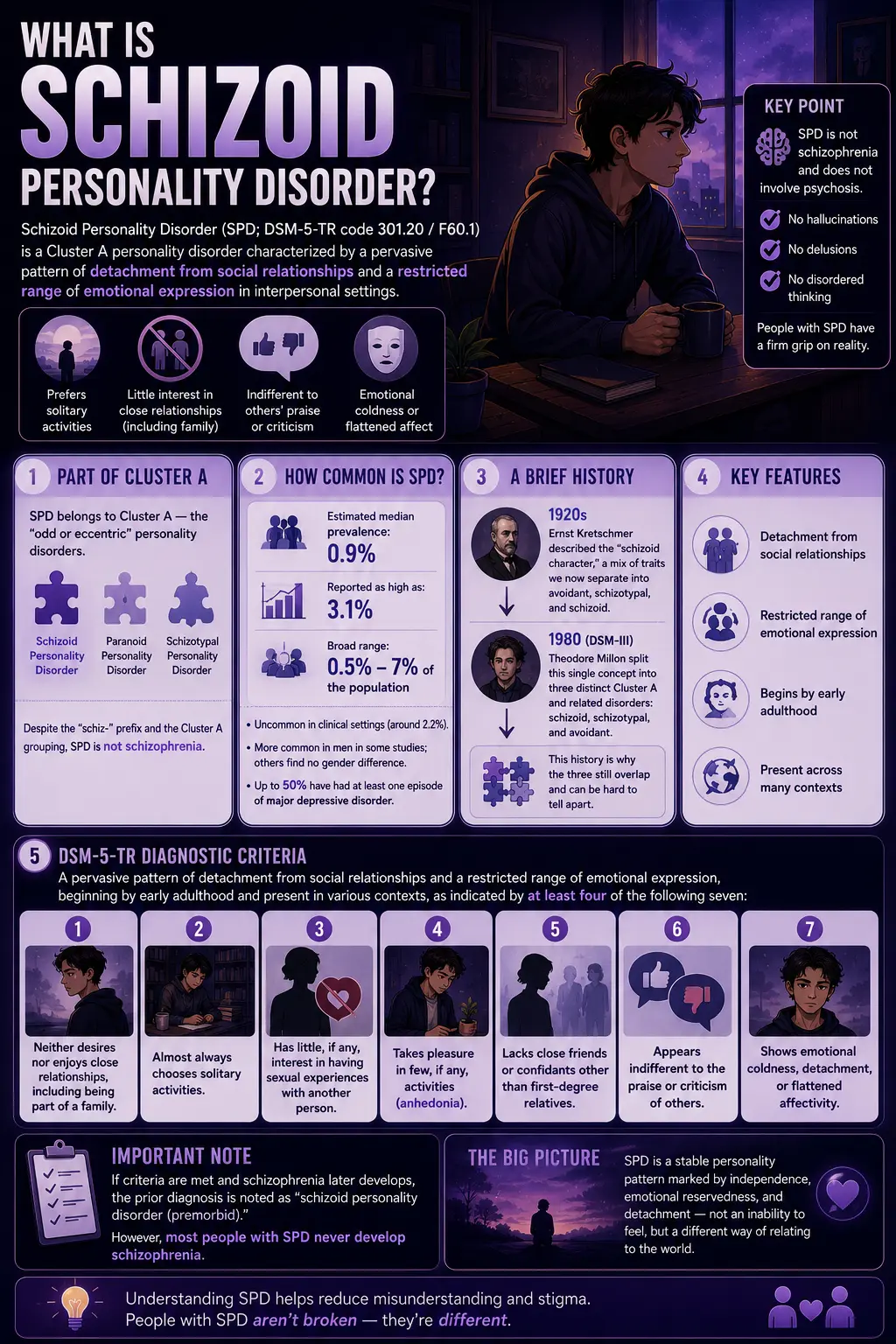
Schizoid Personality Disorder (SPD; DSM-5-TR code 301.20 / F60.1) is a Cluster A personality disorder characterized by a pervasive pattern of detachment from social relationships and a restricted range of emotional expression in interpersonal settings. It begins by early adulthood and is present across many contexts. People with SPD typically prefer solitary activities, have little interest in close relationships (including with family), seem indifferent to others’ praise or criticism, and display emotional coldness or flattened affect.
SPD belongs to Cluster A — the “odd or eccentric” personality disorders — alongside paranoid personality disorder and schizotypal personality disorder. A crucial point: despite the “schiz-” prefix and the Cluster A grouping, SPD is not schizophrenia and does not involve psychosis. People with SPD have a firm grip on reality — no hallucinations, no delusions, no disordered thinking. The shared root reflects a historical and possibly genetic relationship to the schizophrenia spectrum (SPD is more common in families with a history of schizophrenia), but SPD itself is a stable personality pattern, not a psychotic illness.
SPD is relatively uncommon. Prevalence estimates vary widely depending on the criteria used and the population studied: the estimated median is around 0.9%, though some studies report it as high as 3.1% (Merck Manual, 2026), with the broadest range spanning roughly 0.5% to 7% of the population (Wikipedia). It is uncommon in clinical settings (around 2.2%), in part because people with SPD rarely seek treatment — their detachment usually isn’t distressing to them, even if it concerns those around them. Some studies suggest SPD is slightly more common in men; others find no gender difference (Merck Manual). Comorbidities are common: up to half of people with SPD have had at least one episode of major depressive disorder.
The concept has a long history. The Austrian psychiatrist Ernst Kretschmer developed the original idea of the “schizoid character” in the 1920s, describing a mix of what we’d now separate into avoidant, schizotypal, and schizoid traits. It was the work of Theodore Millon around 1980 (DSM-III) that split this single concept into the three distinct Cluster A and related disorders we recognize today — schizoid, schizotypal, and avoidant (Wikipedia). This history is why the three still overlap and are sometimes difficult to tell apart.
The full DSM-5-TR diagnostic criteria require a pervasive pattern of detachment from social relationships and a restricted range of emotional expression, beginning by early adulthood and present in various contexts, as indicated by at least four of the following seven (APA, 2022):
- Neither desires nor enjoys close relationships, including being part of a family.
- Almost always chooses solitary activities.
- Has little, if any, interest in having sexual experiences with another person.
- Takes pleasure in few, if any, activities (anhedonia).
- Lacks close friends or confidants other than first-degree relatives.
- Appears indifferent to the praise or criticism of others.
- Shows emotional coldness, detachment, or flattened affectivity.
If criteria are met and schizophrenia later develops, the prior diagnosis is noted as “schizoid personality disorder (premorbid)” — though most people with SPD never develop schizophrenia.
Signs You Might Have Schizoid Personality Disorder
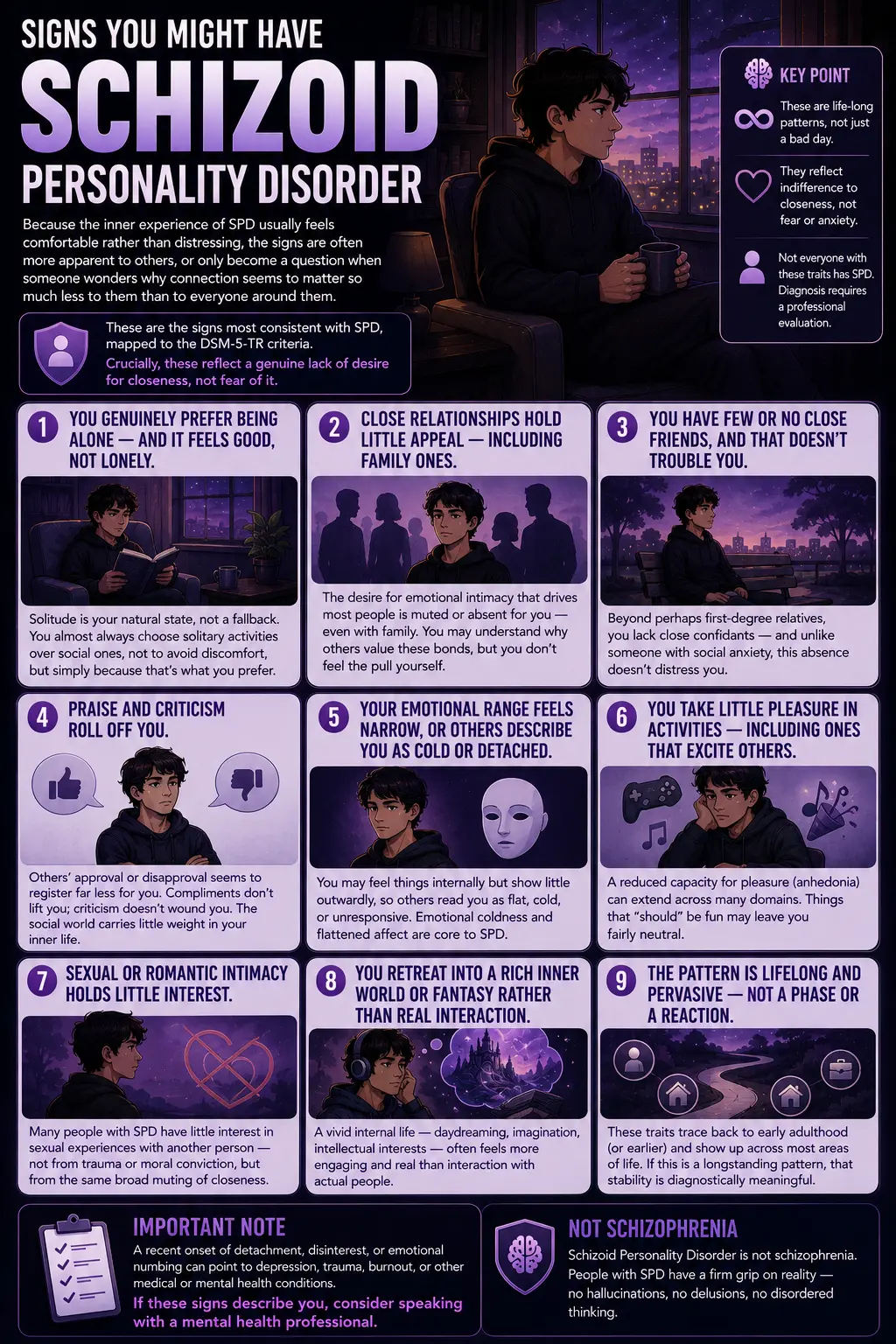
Because the inner experience of SPD usually feels comfortable rather than distressing, the signs are often more apparent to others, or only become a question when someone wonders why connection seems to matter so much less to them than to everyone around them. These are the signs most consistent with SPD, mapped to the DSM-5-TR criteria. Crucially, these reflect a genuine lack of desire for closeness, not fear of it.
You genuinely prefer being alone — and it feels good, not lonely. Solitude is your natural state, not a fallback. Where others feel the absence of company as loneliness, you experience time alone as comfortable and complete. You almost always choose solitary activities over social ones, not to avoid discomfort, but simply because that’s what you prefer.
Close relationships hold little appeal — including family ones. The desire for emotional intimacy that drives most people’s lives is muted or absent for you. This isn’t limited to strangers or acquaintances; it can extend to family and the few people who are typically closest. You may recognize, intellectually, that others value these bonds intensely — but you don’t feel the pull yourself.
You have few or no close friends, and that doesn’t trouble you. Beyond perhaps first-degree relatives, you lack close confidants — and unlike someone with social anxiety, this absence doesn’t distress you. You’re not lonely for a connection you can’t access; you simply don’t seek it.
Praise and criticism roll off you. Others’ approval or disapproval seems to register far less for you than for most people. Compliments don’t particularly lift you; criticism doesn’t particularly wound you. This indifference to others’ evaluations is one of the more distinctive SPD features — it reflects how little weight the social world carries in your inner life.
Your emotional range feels narrow, or others describe you as cold or detached. You may experience your emotional life as muted — fewer highs and lows than others seem to have. Or you may feel things internally but show little outwardly, so others read you as flat, cold, or unresponsive. Emotional coldness and flattened affect are core to SPD.
You take little pleasure in activities — including ones that excite others. A reduced capacity for pleasure (anhedonia) can extend across many domains, including those most people find reliably enjoyable. Things that “should” be fun may leave you fairly neutral.
Sexual or romantic intimacy holds little interest. Many people with SPD have little interest in sexual experiences with another person — not from trauma or moral conviction, but from the same broad muting of the drive toward interpersonal closeness.
You retreat into a rich inner world or fantasy rather than real interaction. Some people with SPD have a vivid internal life — daydreaming, imagination, intellectual interests — that feels more engaging and real than interaction with actual people. The inner world becomes where life is genuinely lived.
The pattern is lifelong and pervasive — not a phase or a reaction. SPD, like all personality disorders, is enduring and stable. These traits trace back to early adulthood (or earlier) and show up across most areas of life, rather than appearing suddenly or only in specific situations. If this describes a longstanding pattern rather than a recent change, that stability is diagnostically meaningful. (A recent onset of detachment, by contrast, can point to depression, trauma, or other conditions and is worth discussing with a professional.)
Schizoid vs Avoidant vs Schizotypal vs Autism
| Feature | Schizoid PD | Avoidant PD | Schizotypal PD | Autism Spectrum |
|---|---|---|---|---|
| Desire for relationships | Genuinely doesn’t desire closeness | Strongly desires closeness but fears rejection | Limited desire, plus discomfort from distorted perceptions | Often desires connection but struggles with social mechanics |
| Why social withdrawal? | Disinterest and detachment | Fear of embarrassment, rejection, criticism | Social anxiety plus odd beliefs/perceptions | Social communication differences, sensory overload |
| Perceptual/cognitive distortions | None | None | Present — odd beliefs, magical thinking, ideas of reference | None (different cognitive profile, not distortions) |
| Emotional expression | Flat, cold, restricted | Anxious, longing, self-critical — emotions present | Constricted or inappropriate affect | Present but may be expressed/read differently |
| Distress about isolation | Little or none — content alone | Significant — wants connection, suffers without it | Variable | Variable — many desire connection |
| PsyMed test | This test | Avoidant PD Test | Schizotypal PD Test | Autism Test |
The single most important distinction is schizoid versus avoidant, because both produce social isolation but for opposite reasons. In SPD, the isolation comes from genuine detachment and disinterest — the person doesn’t particularly want close relationships. In avoidant personality disorder, the isolation comes from a deep desire for connection blocked by an intense fear of rejection and embarrassment (Merck Manual). One person is content alone; the other is painfully lonely. The behaviors can look similar from outside, but the inner experience is completely different — and so is the treatment.
The schizoid versus schizotypal distinction comes down to perceptual and cognitive distortions: schizotypal personality disorder adds odd beliefs, magical thinking, unusual perceptual experiences, and ideas of reference that are entirely absent in SPD. Schizotypal sits closer to the schizophrenia spectrum; schizoid is “purer” detachment without the oddness of thought.
Understanding Your Schizoid Personality Disorder Test Score
A note before your result: this score reflects how strongly your answers align with schizoid traits — it is a starting point for reflection, not a diagnosis. Personality disorders are diagnosed by professionals based on a pervasive, lifelong pattern that causes meaningful difficulty. Many people have some schizoid traits without having the disorder, and a genuine, contented preference for solitude is not something that needs fixing.
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 16 | Minimal — Few Schizoid Indicators | Few schizoid traits indicated. A normal preference for some solitude may be present without the pervasive detachment and emotional restriction of SPD. |
| 17 – 32 | Mild — Some Schizoid Traits | Some schizoid traits present. This may reflect strong introversion or a genuine preference for solitude rather than a disorder. Worth reflecting on whether it causes you difficulty. |
| 33 – 48 | Moderate — Significant Schizoid Traits | A notable pattern of detachment and emotional restriction. If it’s causing difficulty in areas of life you care about, a professional conversation may help. |
| 49 – 64 | High — Strong Schizoid Indicators | Strong alignment with schizoid traits across multiple criteria. A professional evaluation can clarify whether this reflects SPD and whether any support would be useful to you. |
What Causes Schizoid Personality Disorder?
The causes of SPD aren’t fully established, but research points to a combination of genetic and early environmental factors. SPD is more common in people with a family history of schizophrenia or schizotypal personality disorder, suggesting a shared genetic vulnerability along the broader schizophrenia spectrum (Merck Manual). This doesn’t mean SPD leads to schizophrenia — most people with SPD never develop a psychotic disorder — but the familial link is one of the more consistent findings.
Early environmental factors are also implicated. Childhoods marked by emotional coldness, neglect, or emotionally unavailable or detached caregiving appear more frequently in the histories of people with SPD. One developmental understanding is that profound early detachment can become a stable adaptation: if closeness was never warm, available, or rewarding, the developing person may settle into a self-sufficient detachment that persists into adulthood. Temperament likely plays a role too — some people appear to be constitutionally low in the drive for social connection and reward.
SPD is among the more stable personality patterns over time — a two-year follow-up found schizoid and antisocial traits showed the highest stability of the personality disorders studied (StatPearls). It is unlikely to resolve on its own, though addressing comorbidities (especially depression) and improving quality-of-life factors can meaningfully help.
Treatment for Schizoid Personality Disorder
People with SPD rarely seek treatment for the disorder itself, since the detachment usually isn’t distressing to them — they more often come to treatment for a comorbid issue such as depression, or at the urging of family. When treatment does happen, the general principles are the same as for other personality disorders, though the evidence base is thin: notably, no controlled studies of psychotherapy or medication specifically for SPD have been published (Merck Manual).
Psychotherapy. Cognitive Behavioral Therapy is the most commonly used approach. Because forming a therapeutic relationship is itself difficult for someone with SPD, effective therapy tends to move slowly, respect the person’s need for distance, and focus on concrete, agreed goals rather than pushing for emotional intimacy the person doesn’t want. Goals are often practical — reducing isolation where it’s causing problems, building specific social skills, addressing anhedonia — rather than transforming the person into someone who craves connection.
Treating comorbidities. Since up to half of people with SPD experience major depression, and anxiety and other conditions are common, treating these comorbid conditions is frequently the most impactful intervention. There is no medication for SPD itself, but medications may help co-occurring depression or anxiety.
A note on respect and goals. An important and humane point: for many people with strong schizoid traits, a solitary, low-social life is genuinely their preference and not a problem to be fixed. The goal of any support is not to force connection on someone who doesn’t want it, but to address genuine distress or impairment — and to distinguish a contented, self-sufficient solitary life (which needs no treatment) from detachment that is causing real problems the person actually wants to change.
Frequently Asked Questions
What is schizoid personality disorder?
Schizoid Personality Disorder (SPD; DSM-5-TR 301.20 / F60.1) is a Cluster A personality disorder defined by a pervasive pattern of detachment from social relationships and a restricted range of emotional expression, beginning by early adulthood. People with SPD prefer solitary activities, have little desire for close relationships (including family), appear indifferent to praise or criticism, and show emotional coldness or flattened affect. Diagnosis requires at least four of seven DSM-5-TR criteria. Critically, SPD does not involve psychosis — people with SPD have a firm grip on reality — and it differs from introversion or simply enjoying solitude by its pervasiveness, its emotional flatness, and the genuine lack of desire for closeness.
What is the difference between schizoid personality disorder and being introverted?
Introversion is a normal, healthy personality trait — introverts find social interaction draining and need solitude to recharge, but they typically still want and enjoy close relationships, value their friendships, and have a normal range of emotions. Schizoid Personality Disorder is a clinical condition involving a genuine lack of desire for close relationships, restricted emotional expression (emotional coldness or flatness), indifference to others’ opinions, and often reduced pleasure across activities. The key differences: introverts want connection (just in smaller doses); people with SPD largely don’t. Introverts have a full emotional life; SPD involves a muted one. Introversion causes no impairment, whereas SPD is a pervasive pattern that can interfere with functioning. Most quiet, solitary people are simply introverts, not schizoid.
Is schizoid personality disorder the same as schizophrenia?
No. Despite the similar names and shared “schiz-” root, they are distinct. Schizophrenia is a psychotic disorder involving hallucinations, delusions, and disordered thinking. Schizoid Personality Disorder is a personality disorder involving social detachment and emotional restriction, with no psychosis — people with SPD have a clear, accurate grip on reality. The names share a root because of a historical and possibly genetic relationship to the schizophrenia spectrum (SPD is more common in families with schizophrenia), but SPD is not a mild form of schizophrenia and usually does not develop into it. If schizophrenia does later develop in someone with prior SPD, the personality disorder is then noted as “premorbid.”
What is the difference between schizoid and avoidant personality disorder?
This is the most important distinction, because both cause social isolation but for opposite reasons. In Schizoid Personality Disorder, the person genuinely does not desire close relationships — they are content alone, and their isolation isn’t distressing to them. In Avoidant Personality Disorder, the person deeply wants close relationships but avoids them out of intense fear of rejection, criticism, and embarrassment — their isolation is painful and unwanted. From the outside, both may look like a withdrawn loner; on the inside, one is content, and the other is lonely and longing. The treatments differ accordingly: avoidant PD work focuses on the fear of rejection, while SPD work (when wanted) focuses on practical functioning without forcing unwanted intimacy.
How common is schizoid personality disorder?
SPD is relatively uncommon, though estimates vary widely depending on the criteria used and the population studied. The estimated median prevalence is around 0.9%, with some studies finding rates as high as 3.1% (Merck Manual), and the broadest range across studies spanning roughly 0.5% to 7%. It’s uncommon in clinical settings (around 2.2%), largely because people with SPD seldom seek treatment — the detachment usually doesn’t distress them. Some research suggests it’s slightly more common in men, while other studies find no gender difference. It is more common among people with a family history of schizophrenia or schizotypal personality disorder.
Can schizoid personality disorder be treated?
It can be addressed, though the evidence base is limited — no controlled studies of therapy or medication specifically for SPD have been published. Cognitive Behavioral Therapy is the most commonly used approach, typically moving slowly, respecting the person’s need for distance, and focusing on concrete goals rather than forcing emotional intimacy. Because up to half of people with SPD experience major depression, treating comorbid conditions is often the most impactful intervention. Importantly, treatment is not about turning a solitary person into a social one against their wishes — for many people, a low-social life is a genuine preference, not a problem. Treatment targets genuine distress or impairment that the person actually wants to change.
Do people with schizoid personality disorder have emotions?
Yes, though their emotional life is typically muted and their outward expression restricted. People with SPD often experience a narrower range of emotion than most people, with fewer intense highs and lows, and they tend to show little emotion outwardly, which others may read as coldness or indifference. Some people with SPD describe a rich inner world of thought, imagination, and intellectual interest even alongside flat outward affect and emotional distance in relationships. The “emotional coldness” of SPD is real, but it doesn’t mean a complete absence of inner experience — it means a restricted range and limited expression, particularly in interpersonal contexts.
Related Tests
- Avoidant Personality Disorder Test — the most important differential; avoidant PD also causes social isolation, but from fear of rejection rather than genuine disinterest in closeness.
- Schizotypal Personality Disorder Test — the Cluster A relative that adds odd beliefs, magical thinking, and perceptual distortions, absent in schizoid PD.
- Paranoid Personality Disorder Test — the third Cluster A disorder; shares social detachment but is driven by distrust and suspicion of others.
- Social Anxiety Test — social anxiety can resemble schizoid withdrawal, but the underlying fear of judgment distinguishes it from genuine schizoid disinterest.
- Clinical Depression Test — depression can cause social withdrawal and anhedonia that mimic SPD; up to half of people with SPD also experience major depression.
- All Personality Disorder Tests — explore the full set of Cluster A, B, and C personality disorder screenings.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Schizoid Personality Disorder 301.20 (F60.1), pp. 741–744. psychiatry.org
- Merck Manual Professional Edition. (2026). Schizoid Personality Disorder (ScPD). [Prevalence ~0.9-3.1%; criteria; CBT; ~50% comorbid MDD; no controlled treatment studies] merckmanuals.com
- Esterberg, M.L., Goulding, S.M., & Walker, E.F. (2010); StatPearls (2024). Schizoid Personality Disorder. [Prevalence; stability; comorbidity; Kretschmer/Millon history; premorbid specifier] ncbi.nlm.nih.gov
- EBSCO Research Starters. (2025). Schizoid personality disorder (SPD). [Seven DSM-5-TR criteria; Cluster A; Bleuler/Kretschmer history] ebsco.com
- Wikipedia. (2026). Schizoid personality disorder. [Kretschmer 1920s schizoid character; Millon 1980 split; prevalence range 0.5-7%; diagnostic debate] en.wikipedia.org
- Millon, T. (1981). Disorders of Personality: DSM-III, Axis II. Wiley. [Splitting the schizoid character into schizoid, schizotypal, avoidant, schizoid subtypes]
- Triebwasser, J., Chemerinski, E., Roussos, P., & Siever, L.J. (2012). Schizoid personality disorder. Journal of Personality Disorders, 26(6), 919–926. [Construct validity debate; proposed dimensional model]