A persistent pattern of disregard for the rights of others. That’s the clinical definition of Antisocial Personality Disorder — and, like most clinical definitions, it significantly understates the texture of the experience.
It isn’t simply about being difficult or self-interested. It’s a pattern that shows up consistently across different situations and different relationships: rules feel like obstacles for people who need them. Honesty is a tool deployed when useful, not a default. Other people’s distress registers intellectually, but doesn’t carry the emotional weight needed to change behavior. Consequences — when they come — don’t produce the learning they seem to produce in others.
This free Antisocial Personality Disorder Test screens for ASPD using all seven diagnostic criteria from the DSM-5-TR (APA, 2022) — the same framework used in formal clinical evaluations. 15 questions. Instant, private results.
This is a screening tool, not a clinical diagnosis. But it is based on real diagnostic criteria, and a significant score warrants seeing a mental health professional who can conduct a proper assessment.
What Is Antisocial Personality Disorder (ASPD)?
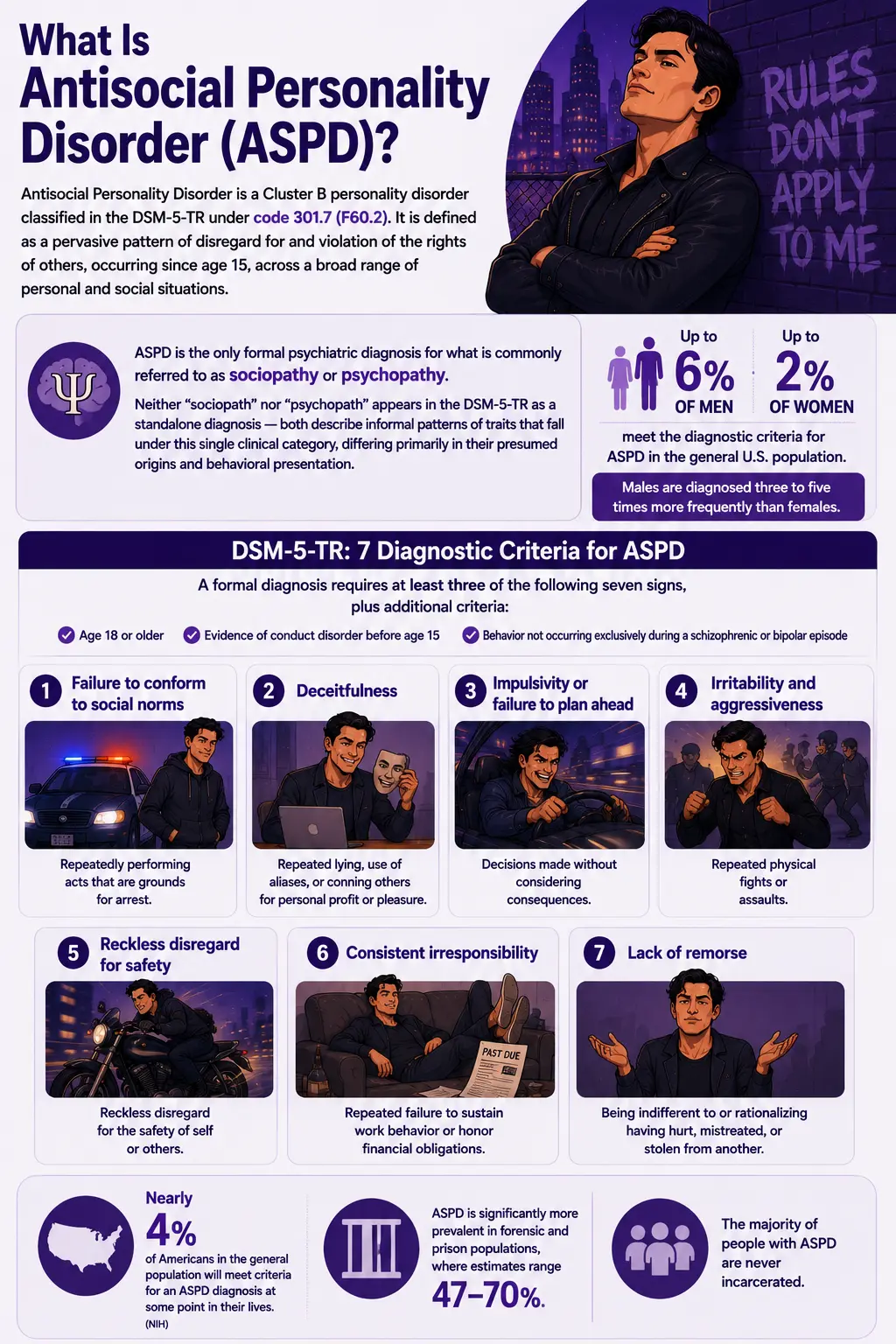
Antisocial Personality Disorder is a Cluster B personality disorder classified in the DSM-5-TR under code 301.7 (F60.2). It is defined as a pervasive pattern of disregard for and violation of the rights of others, occurring since age 15, across a broad range of personal and social situations.
ASPD is the only formal psychiatric diagnosis for what is commonly referred to as sociopathy or psychopathy. Neither “sociopath” nor “psychopath” appears in the DSM-5-TR as a standalone diagnosis — both describe informal patterns of traits that fall under this single clinical category, differing primarily in their presumed origins and behavioral presentation.
The DSM-5-TR specifies seven diagnostic criteria for ASPD. A formal diagnosis requires at least three of the following seven signs, plus additional criteria, including age 18 or older, evidence of conduct disorder before age 15, and the behavior not occurring exclusively during a schizophrenic or bipolar episode:
- Failure to conform to social norms — repeatedly performing acts that are grounds for arrest.
- Deceitfulness — repeated lying, use of aliases, or conning others for personal profit or pleasure.
- Impulsivity or failure to plan ahead — decisions made without considering consequences.
- Irritability and aggressiveness — repeated physical fights or assaults.
- Reckless disregard for safety — of self or others.
- Consistent irresponsibility — repeated failure to sustain work behavior or honor financial obligations.
- Lack of remorse — being indifferent to or rationalizing having hurt, mistreated, or stolen from another.
Nearly 4% of Americans in the general population will meet criteria for an ASPD diagnosis at some point in their lives (NIH). Up to 6% of men and 2% of women meet the diagnostic criteria for ASPD in the general U.S. population — males are diagnosed three to five times more frequently than females. ASPD is significantly more prevalent in forensic and prison populations, where estimates range from 47–70%, though the majority of people with ASPD are never incarcerated.
ASPD Symptoms — What Antisocial Personality Disorder Actually Looks Like
ASPD is frequently mischaracterized in popular media as dramatic villainy. The clinical presentation is typically more mundane — and in many ways more functional-looking than people expect. People with ASPD often present as charming, confident, and verbally skilled. The disorder reveals itself over time and across contexts, not in a single encounter.
Pervasive disregard for rules and social norms
Not occasional rule-breaking under pressure — a sustained, pattern-level indifference to legal, social, and ethical constraints that most people experience as genuinely binding. This can manifest as repeated criminal activity, systematic exploitation of loopholes, or simply a settled sense that the rules governing other people’s behavior don’t apply equally to them.
Chronic deceitfulness
Lying, conning, and manipulation are not exceptional tactics — they are default instruments used fluidly across relationships, professional settings, and any context where they serve a purpose. The deception tends to feel natural rather than guilt-producing. People with ASPD are often skilled at reading what others need to hear and providing it convincingly.
Impulsivity and poor future orientation
Decisions are made quickly, without adequate consideration of downstream consequences. There is a pattern of moving between situations — jobs, relationships, cities, plans — without sustained engagement. The future feels less real and less motivating than the present.
Irritability and aggression
A consistently low threshold for provocation. When challenged, disrespected, or frustrated, the response can be verbal aggression, intimidation, or physical confrontation. The aggression is not always overt — it can operate through calculated social destruction, retaliation, or sustained pressure.
Reckless disregard for safety
An underweighting of consequences to self and others in risk-taking decisions — financial, physical, relational. This is not courage or adventurousness. It is a genuine reduction in the weight assigned to safety in decision-making.
Consistent irresponsibility
Repeated failure to meet sustained obligations: financial commitments not honored, employment not maintained, relational responsibilities not fulfilled. The pattern is not one of failure through effort — it is failure through disengagement.
Absence of genuine remorse
The core affective feature. When harm is done, the response is indifference, rationalization, or brief acknowledgment without lasting impact on future behavior. Remorse, when it appears, is typically instrumental — managing someone else’s reaction — rather than genuine. The harm done registers intellectually. It doesn’t carry the emotional weight that produces change.

ASPD vs. Sociopathy vs. Psychopathy — Clarifying the Relationship
These terms are used interchangeably in everyday language and incorrectly in most online content. The clinical picture is important to understand accurately, particularly for anyone trying to understand a formal diagnostic context.
| Feature | ASPD (DSM-5-TR) | Sociopathy (informal) | Psychopathy (informal/PCL-R) |
|---|---|---|---|
| Formal diagnosis | Yes — DSM-5-TR 301.7 / F60.2 | No — informal term for ASPD subtype | No — assessed via PCL-R, not DSM |
| Relationship to each other | Umbrella diagnosis covering both | More impulsive, erratic ASPD pattern | More calculated, emotionally shallow ASPD pattern |
| Primary assessment tool | DSM-5-TR structured clinical interview | DSM-5-TR ASPD criteria | Hare PCL-R (Psychopathy Checklist-Revised) |
| Conduct disorder required | Yes — before age 15 | Yes — part of ASPD criteria | Not formally required by PCL-R |
| Emotional profile | Spectrum — from limited to profound emotional deficits | May retain limited emotional connections | Profound shallow affect — empathy largely absent |
| Prevalence | 1–4% general population; up to 70% in prison | Subset of ASPD | ~1% general population |
For the sociopathy-specific trait assessment, our Sociopath Test covers the experiential and behavioral patterns in depth. For the psychopathy-specific PCL-R assessment, our Psychopath Test covers all four PCL-R facets.
ASPD and Conduct Disorder — The Developmental Link
One of the most clinically important and least publicly understood features of ASPD is the requirement for a history of conduct disorder before age 15. This isn’t an arbitrary rule — it reflects the DSM-5-TR’s understanding of ASPD as a developmental disorder with roots in early life, not a condition that emerges suddenly in adulthood.
Conduct disorder in childhood involves a persistent pattern of violating others’ rights and breaking social rules: aggression toward people or animals, destruction of property, deceitfulness or theft, and serious rule violations. Not every child with conduct disorder develops ASPD, but ASPD cannot be diagnosed without evidence of this early pattern.
Adults who display all ASPD criteria but without documented childhood conduct disorder may be classified as adult antisocial behavior (a V/Z code in the DSM-5-TR and ICD) rather than formal ASPD. This distinction matters clinically but may not be meaningful in everyday assessment — the behavioral pattern carries consequences regardless of the formal label.
What Causes Antisocial Personality Disorder?
ASPD is a multifactorial condition shaped by the interaction of genetic predisposition, neurobiological differences, and developmental experience. No single factor explains it — and the relative contribution of each varies significantly across individuals.
Genetic predisposition
Twin studies consistently demonstrate significant heritability for ASPD and antisocial behavior broadly. Having a first-degree relative with ASPD, substance use disorder, or conduct disorder substantially elevates risk. Specific genetic contributions relate to impulse control, emotional reactivity, and reward processing — not antisocial behavior directly, but the neurological substrates that increase its likelihood.
Neurobiological factors
Consistent structural and functional brain differences have been identified in ASPD and psychopathic presentations: reduced amygdala volume and reactivity (underlying the reduced fear response and empathy deficit), reduced prefrontal cortex activity (underlying impaired impulse control and future orientation), and altered connectivity between these regions. These findings are more pronounced in the psychopathic subgroup but present across the ASPD spectrum.
Early adverse experiences
Childhood abuse, neglect, unpredictable or violent home environments, and early exposure to criminality all significantly elevate ASPD risk. These experiences interact with genetic predisposition to shape the development of emotion regulation, empathy, and attachment — often in ways that are adaptive in early, chaotic environments but become maladaptive in stable adult contexts.
Conduct disorder as the precursor
As noted, ASPD requires conduct disorder before age 15. The developmental pathway from conduct disorder to ASPD is not inevitable — protective factors, including stable caregiving, educational engagement, and early therapeutic intervention, can interrupt it. But the earlier and more severe the conduct disorder, the higher the ASPD risk.
Comorbid conditions
Patients with antisocial personality disorder often also have an impulse control disorder, mood disorders, anxiety disorders, gambling disorder, attention-deficit/hyperactivity disorder, or borderline personality disorder. Substance use disorders are particularly common — the impulsivity and reward-seeking of ASPD create significant vulnerability to addiction, and substance use further disinhibits antisocial behavior.
How This Antisocial Personality Disorder Test Works
This test directly maps to all seven DSM-5-TR ASPD diagnostic criteria, supplemented by the core affective and interpersonal features most consistently associated with ASPD in the clinical literature (callousness, empathy deficit, entitlement, manipulativeness). Every question reflects a recognized clinical feature — nothing is speculative or based on popular misconceptions.
Answer based on your consistent pattern across your life — not your best day, and not a single incident. The scale is:
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. Results are instant and completely private.
Understanding Your ASPD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few ASPD Indicators | Responses suggest few significant ASPD trait patterns. Self-interest and occasional rule-bending are part of normal human variation and don’t indicate ASPD at this level. |
| 16 – 30 | Mild — Some Patterns Present | Some ASPD-related patterns are present. These may reflect subclinical traits, specific circumstances, or co-occurring conditions. Worth exploring with a professional. |
| 31 – 45 | Moderate — Significant ASPD Pattern | Multiple ASPD indicators are present across several diagnostic domains. This pattern is consistent with meaningful antisocial personality features. A clinical evaluation is strongly recommended. |
| 46 – 60 | High — Strong ASPD Indicators | Strong, pervasive ASPD patterns are indicated across multiple diagnostic criteria. A formal clinical evaluation by a mental health professional is strongly recommended. |
Can Antisocial Personality Disorder Be Treated?
ASPD has historically been described as one of the most treatment-resistant personality disorders. That reputation is partly deserved — the ego-syntonic nature of many traits, low intrinsic motivation for change, frequent co-occurring substance use, and high dropout rates from treatment all create real challenges. But the clinical picture is more nuanced than “untreatable,” and this view is actively shifting in the research literature.
Schema Therapy
Currently, the most evidence-supported treatment for ASPD. Schema Therapy identifies the early maladaptive schemas — deeply held, largely unconscious beliefs about self, others, and the world — that drive antisocial behavior, and works systematically to address them through a combination of cognitive, experiential, and relational techniques. It has shown meaningful outcomes in both community and forensic populations.
Mentalization-Based Treatment (MBT)
Developed by Peter Fonagy, MBT targets the capacity to understand mental states — to think about what’s happening in one’s own mind and others’. Research shows that MBT can improve mentalizing capacity in individuals with significant antisocial features, leading to downstream improvements in interpersonal behavior.
Reasoning and Rehabilitation (R&R) Program
A structured CBT-based intervention specifically developed for antisocial populations — originally in forensic settings. R&R targets cognitive distortions, impulse control, problem-solving, and perspective-taking. It has the strongest evidence base for reducing reoffending in forensic ASPD populations specifically.
Treating co-occurring conditions
The most consistent finding in ASPD outcome research is that treating co-occurring substance use, depression, anxiety, and ADHD produces meaningful reductions in overall antisocial behavior — even when the underlying ASPD proves resistant to direct treatment. These conditions substantially compound the disorder, and their treatment matters.
The age factor
One of the most consistent findings in longitudinal ASPD research is that antisocial behavior tends to decrease with age — the phenomenon sometimes called “burning out.” Rates of aggressive and impulsive behavior are significantly lower in people with ASPD over 40 than in younger adults with the same diagnosis. The affective features show less change, but functional improvement across domains is achievable.
Frequently Asked Questions
What is Antisocial Personality Disorder?
Antisocial Personality Disorder (ASPD) is a Cluster B personality disorder (DSM-5-TR 301.7 / F60.2) defined as a pervasive pattern of disregard for and violation of the rights of others, beginning in childhood or early adolescence and persisting into adulthood. A formal diagnosis requires at least 3 of 7 specified criteria, evidence of conduct disorder before age 15, and being age 18 or older. Nearly 4% of Americans will meet ASPD criteria at some point in their lives, with men diagnosed three to five times more frequently than women. ASPD is the only formal psychiatric diagnosis covering what is informally called sociopathy or psychopathy.
What are the signs of Antisocial Personality Disorder?
The seven DSM-5-TR signs of ASPD are: failure to conform to social norms regarding lawful behavior, deceitfulness and manipulation for personal gain, impulsivity or failure to plan ahead, irritability and aggressiveness, reckless disregard for the safety of self or others, consistent irresponsibility in work and financial obligations, and lack of remorse for harm done to others. At least three of these seven must be present persistently and pervasively across settings. Onset must trace back to conduct disorder before age 15, and the person must be 18 or older to meet criteria for ASPD.
Is ASPD the same as being a sociopath or psychopath?
ASPD is the only formal DSM-5-TR diagnosis — neither “sociopath” nor “psychopath” is an official diagnostic category. Both terms describe informal subtypes of ASPD that differ in behavioral style and presumed origin: the sociopath pattern is more impulsive and environmentally driven; the psychopath pattern is more calculated, emotionally shallow, and neurobiologically driven. All three labels refer to people who would formally receive the ASPD diagnosis. Our Sociopath Test and Psychopath Test cover these specific patterns in more depth.
Why does ASPD require childhood conduct disorder?
The DSM-5-TR requires evidence of conduct disorder before age 15 because ASPD is understood developmentally as a persistent personality disorder with roots in early life rather than a condition that emerges suddenly in adulthood. This requirement helps distinguish ASPD from antisocial behavior arising from other causes (substance use, situational stress, other psychiatric conditions). Adults who meet all other ASPD criteria but lack documented childhood conduct disorder may be classified under “adult antisocial behavior” (a V/Z code) rather than formal ASPD.
Can someone with ASPD have relationships?
Yes, though the quality and stability of those relationships are typically affected by the disorder. People with ASPD can form attachments and maintain relationships, particularly in early stages when charm, confidence, and social skills are prominent. Over time, patterns of dishonesty, exploitation, irresponsibility, and limited genuine empathy tend to significantly damage relationships. The psychopathic subgroup shows the most severe interpersonal deficits. The sociopathic subgroup may retain limited capacity for emotional connection with specific individuals. With treatment — particularly Schema Therapy — improvements in relational capacity are possible.
How is ASPD formally diagnosed?
No self-assessment, blood test, or imaging exam can diagnose antisocial personality disorder. A formal diagnosis involves a comprehensive clinical evaluation by a psychiatrist or psychologist: structured interviews covering current and historical behavioral patterns, collateral information where available, a review of childhood history for conduct disorder, a mental status examination, and ruling out other conditions. Most people who experience antisocial personality disorder don’t seek a diagnosis on their own — a mental health evaluation is usually requested by a court of law. This screening is a starting point for a conversation with a professional — not a substitute for formal assessment.
Related Tests
ASPD sits within a broader cluster of personality disorder and trait assessments. These are the most clinically relevant:
- Sociopath Test — the experiential trait assessment for the sociopathic presentation of ASPD; covers the behavioral and emotional pattern in depth
- Psychopath Test — the PCL-R four-facet assessment for the psychopathic presentation; a more calculated, emotionally shallow pattern
- Dark Triad Test — screens for Narcissism, Machiavellianism, and Psychopathy together; the combination is most predictive of interpersonal harm
- Narcissistic Personality Disorder Test — NPD and ASPD share manipulation, entitlement, and lack of empathy; they frequently co-occur
- Cluster B Personality Disorder Test — broader screening across all four Cluster B disorders: ASPD, NPD, BPD, and HPD
- ADHD Test — ADHD and ASPD share impulsivity and inconsistency; they co-occur at clinically meaningful rates, and the distinction affects treatment
For the full range of personality disorder screenings, visit our Personality Disorders collection.
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). 301.7 (F60.2) Antisocial Personality Disorder. psychiatry.org
- StatPearls. (2024). Antisocial Personality Disorder. ncbi.nlm.nih.gov
- eCare Behavioral Health Institute. (2025). 22 Antisocial Personality Disorder Statistics for 2025. ecarebehavioralinstitute.com
- Merck Manual Professional Edition. (2026). Antisocial Personality Disorder (ASPD). merckmanuals.com
- American Psychiatric Association. (2023). Antisocial Personality Disorder: Often Overlooked and Untreated. psychiatry.org
- Cleveland Clinic. (2025). Antisocial Personality Disorder (ASPD): Symptoms & Treatment. my.clevelandclinic.org
- Gori, A., et al. (2025). Clinicians’ Assessment of Antisocial Personality Disorder: A Network Analysis Approach on DSM-5-TR Criteria. Personality and Mental Health. onlinelibrary.wiley.com
- PubMed. (2024). Antisocial Personality Disorder. pubmed.ncbi.nlm.nih.gov