
The need to be seen is human. Everyone wants to be noticed, appreciated, and admired on occasion. But for most people, this need is intermittent — it ebbs and flows, and its absence is tolerable. For others, the need is constant and urgent. Not being the center of attention is not just uncomfortable — it is intolerable. The emotions in the room should be moving in your direction. The performance continues whether or not you consciously choose it, because the alternative — being ordinary, unremarkable, unnoticed — is a state you cannot sustain.
Histrionic Personality Disorder is the Cluster B condition most frequently mischaracterized as simply dramatic personality or attention-seeking behavior. It is more clinically specific than those descriptions suggest: a pervasive, enduring pattern of excessive emotionality and attention-seeking that affects multiple domains of life — relationships, work, self-presentation, and the interpretation of intimacy — and causes meaningful functional impairment. It is not a performance choice. It is a personality structure.
This free Histrionic Personality Disorder Test screens for HPD using all 8 DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Based on the past 12 months. Instant, private results.
What Is Histrionic Personality Disorder?
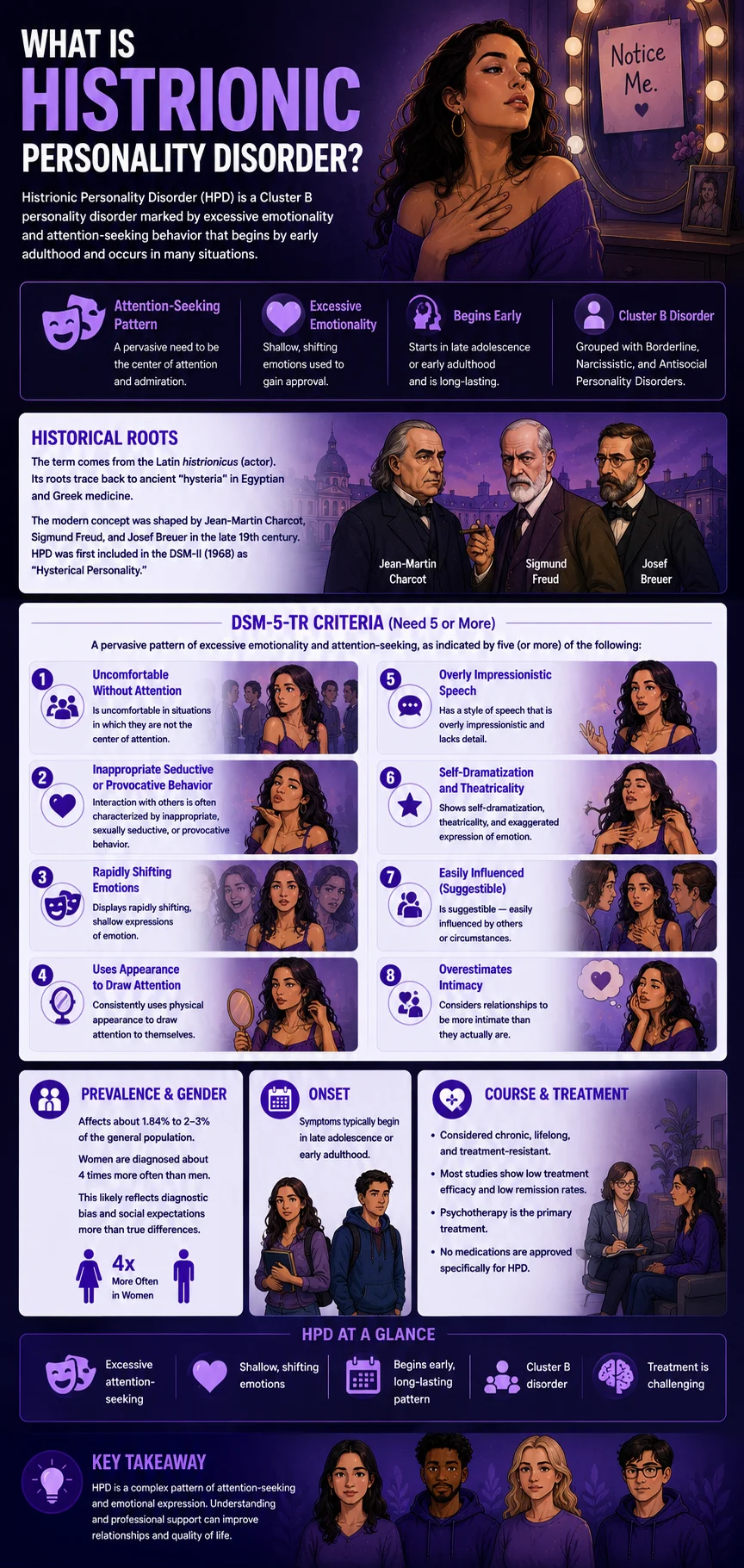
Histrionic Personality Disorder (HPD) is a Cluster B personality disorder (DSM-5-TR code 301.50 / ICD-10: F60.4) — grouped alongside Borderline, Narcissistic, and Antisocial Personality Disorders under the “dramatic, emotional, or erratic” cluster. The DSM-5-TR defines HPD as a pervasive pattern of excessive emotionality and attention-seeking, beginning by early adulthood and present in a variety of contexts (APA, 2022).
The term derives from the Latin histrionicus (actor or performer), itself rooted in the ancient concept of “hysteria” — one of the oldest psychiatric concepts in recorded history, traced to ancient Egyptian and Greek medicine. The modern clinical concept of HPD was shaped by the work of Jean-Martin Charcot at the Salpêtrière in Paris, and by Sigmund Freud and Josef Breuer, whose foundational case studies in the late 19th century helped establish the psychological understanding of the condition (Novais, Araújo & Godinho, Frontiers in Psychology, 2015). HPD was first formally included in the DSM-II (1968) as “Hysterical Personality.”
Prevalence estimates range from approximately 1.84% to 2–3% of the general population (Zimmerman, Rothschild & Chelminski, 2005, cited in Merck Manual, 2026; Meredith Palm / Baylor, 2024). Women are diagnosed approximately four times more often than men, though researchers and the DSM-5-TR note this likely reflects diagnostic bias as much as genuine sex differences — the criteria describe presentation patterns that are more socially permissible for women, and the same behaviors may not be identified or labeled the same way in male patients (APA, 2022; Baylor, 2024). Onset is typically in late adolescence or early adulthood (StatPearls, Torrico, French & Aslam, 2024).
HPD is considered a chronic, lifelong, treatment-resistant condition by StatPearls (Torrico et al., 2024) — with most studies reporting low efficacy for treatment, low rates of symptom remission, and a failure to achieve normative levels of functioning. Psychotherapy is the primary treatment modality, with no specific medications approved for the disorder itself.
The DSM-5-TR requires ≥5 of the following 8 criteria for diagnosis (APA, 2022):
Criterion 1. Is uncomfortable in situations in which they are not the center of attention.
Criterion 2. Interaction with others is often characterized by inappropriate, sexually seductive, or provocative behavior.
Criterion 3. Displays rapidly shifting, shallow expressions of emotion.
Criterion 4. Consistently uses physical appearance to draw attention to themselves.
Criterion 5. Has a style of speech that is overly impressionistic and lacks detail.
Criterion 6. Shows self-dramatization, theatricality, and exaggerated expression of emotion.
Criterion 7. Is suggestible — easily influenced by others or circumstances.
Criterion 8. Considers relationships to be more intimate than they actually are.
Signs You Might Have Histrionic Personality Disorder
HPD is frequently misidentified — both as a positive trait (charisma, expressiveness, social confidence) and as other conditions (narcissism, BPD, bipolar disorder). These are the patterns that most consistently indicate HPD may be present, organized around the 8 DSM-5-TR criteria.
Being unnoticed feels genuinely intolerable — not just uncomfortable. Criterion 1 is the cornerstone of HPD: discomfort when not the center of attention. This is not the ordinary preference for recognition that most people share. It is a structural inability to tolerate not being the focal point — in social groups, in conversations, in relationships. When the room’s attention moves away from you, something urgent and distressing activates. Social situations that don’t produce attention feel wrong, flat, and intolerable.
Your interactions with others are often sexually seductive or provocative — in contexts where this is inappropriate. Criterion 2 is not about sexual attraction or flirtation in appropriate contexts. It is the pattern of seductive or provocative interaction as a default mode across inappropriate contexts — at work, in professional settings, with new acquaintances, in situations where sexual or romantic framing is clearly out of place. Seductiveness is a tool for securing attention and admiration, not primarily an expression of attraction.
Your emotions shift rapidly and feel shallow to others — or to yourself in retrospect. Criterion 3 describes the characteristic emotional style of HPD: emotions that move quickly from one state to another, appear intense in the moment, but resolve or shift before the situation that produced them changes. Others may describe your emotional responses as theatrical, difficult to take seriously, or inconsistent with the actual events. You may notice, retrospectively, that the emotional intensity of a moment dissipated far faster than it would for most people.
You invest significantly in your physical appearance and use it deliberately to draw attention. Criterion 4 is not about caring how you look. It is the habitual, deliberate use of physical appearance as a primary tool for securing attention and admiration — dressing for maximum impact, consistently prioritizing appearance over other considerations, and experiencing marked distress when appearance fails to elicit the expected response.
Your speech is vivid and emotionally expressive but often light on specifics. Criterion 5 describes a characteristic speech pattern: excessively impressionistic, relying on strong adjectives, emotional coloring, and dramatic framing rather than specific facts, concrete details, or supporting reasoning. When asked to substantiate a strong opinion or recall a specific event, the details are vague. The impression dominates the content.
You are theatrical in emotional expression — your reactions feel like performances, even to you. Criterion 6 captures the self-dramatization that characterizes HPD — a tendency to express emotions with theatrical intensity that goes beyond what the situation would ordinarily warrant, and that often strikes observers as performed rather than felt. The person with HPD is not typically calculating the performance; it has become the default mode of emotional expression.
You are easily influenced by other people’s opinions, the latest trend, or the most charismatic person in the room. Criterion 7 — suggestibility — reflects an unusual susceptibility to influence: opinions that shift readily in response to the most recent persuasive voice, beliefs that update based on social pressure rather than evidence, and a general orientation toward external sources for direction about what to think and feel. This is connected to the attention-seeking dynamic: the influencer becomes the source of the validation sought.
You experience relationships as more intimate or significant than the other person does. Criterion 8 documents one of the most painful and consistently misunderstood features of HPD: the tendency to experience relationships as more developed, more mutual, and more intimate than they actually are — and to be repeatedly confused or hurt when others don’t share this assessment. A brief professional acquaintance becomes “a close friend.” A new romantic interest is immediately experienced as a significant partner. The intimacy assessment is systematically inflated.

HPD vs Narcissistic PD vs Borderline PD vs Bipolar Disorder
| Feature | Histrionic PD (HPD) | Narcissistic PD (NPD) | Borderline PD (BPD) | Bipolar Disorder |
|---|---|---|---|---|
| Core motivation | Attention and admiration — being seen, captivated, and entertained by | Recognition of superiority — entitlement to special treatment based on being exceptional | Avoiding abandonment — fear of rejection and emotional annihilation drives behavior | Not personality-driven — episodic mood states (mania/depression) with return to baseline |
| Emotional style | Rapidly shifting, shallow, theatrical — expressed for effect and audience | Controlled presentation; rage when ego threatened; primarily flat between challenges | Intense, dysregulated, genuine — driven by abandonment fear and identity instability | Episodic — normal between mood episodes; episodes involve distinct mood state changes |
| Relationship pattern | Overestimates intimacy; seductive; focused on exciting new connections over sustaining existing ones | Exploitative; idealizes those who validate; devalues those who don’t | Intense, unstable; idealization-devaluation driven by abandonment fear; frantic attempts to avoid real/imagined abandonment | Relationships are affected by mood episodes, but the pattern is not driven by relationship dynamics specifically |
| Self-concept | Dependent on others’ attention and admiration, charming self-presentation is central | Inflated, grandiose; fragile under the surface; entitlement is a stable feature | Unstable, shifting, chronic emptiness, and identity disturbance is a defining features | Not defined by personality features — stable between episodes |
| DSM-5-TR code | 301.50 (F60.4) | 301.81 (F60.81) | 301.83 (F60.3) | 296.xx / 296.89 |
| PsyMed test | This test | NPD Test | BPD Test | Bipolar Test |
An important clinical note on HPD and narcissism: both involve a need for attention and admiration, and both are Cluster B. The critical distinction is the quality of the attention sought. The narcissist seeks validation of their superiority and specialness — they want to be recognized as exceptional. The histrionic person seeks attention itself — the experience of being the focal point, captivated by, and emotionally connected to, the room. The narcissist needs to be the most impressive person in the room; the histrionic person needs to be the most noticed.
What Causes Histrionic Personality Disorder?
The etiology of HPD is not well established compared to other Cluster B disorders, partly because HPD has received less research attention than BPD or NPD. The current evidence supports a multifactorial model.
Developmental origins. HPD is thought to develop from early relational experiences in which the child learned that emotional performance and attention-seeking were the most reliable strategies for obtaining care, validation, and connection. Where ordinary bids for connection were unreliable or insufficient, dramatic escalation of emotional display became the learned strategy. The resulting personality structure is organized around obtaining attention as a primary emotional need (Merck Manual, 2026).
Attachment and parenting patterns. Research links HPD to inconsistent or conditional parenting — where attention and affirmation were available but unpredictable, leading to escalating performance as a strategy for securing them. The child who must perform to receive love develops into the adult who cannot stop performing.
Temperament. Biological temperament features — particularly high emotional reactivity, strong extraversion, and elevated sensitivity to social reward — likely interact with developmental experience to shape HPD. The same temperamental features that, in a supportive developmental environment, produce charisma and social warmth may produce HPD in less supportive conditions.
Comorbidities. HPD has high rates of comorbidity with other Cluster B personality disorders — particularly BPD and NPD. Major depressive disorder is common — people with HPD often become depressed when they are not the center of attention (Merck Manual, 2026). Anxiety disorders and somatic symptom disorders are also associated. The Dependent Personality Disorder profile shares significant overlap — both involve high dependency on others’ approval, though through different expressions.

How This Test Works
This Histrionic Personality Disorder Test covers all 8 DSM-5-TR diagnostic criteria for HPD across 15 questions — attention-seeking, seductiveness, emotional shallowness and lability, use of appearance, impressionistic speech, self-dramatization, suggestibility, and the overestimation of relationship intimacy — as well as functional impact and chronicity.
The HPD test can be completed for yourself or answered with someone in your life in mind. Answer based on your consistent pattern over the past 12 months — not your best or worst days, but the recurring pattern.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. This is a screening tool. Only a qualified mental health professional can diagnose HPD through comprehensive clinical assessment.
Understanding Your Histrionic Personality Disorder Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few HPD Indicators | Few significant HPD patterns present. Occasional attention-seeking or emotional expressiveness may be present within the normal range without a pattern consistent with HPD. |
| 16 – 30 | Mild — Some Histrionic Patterns Present | Some histrionic features present across multiple domains. Below the clinical threshold, but patterns are meaningful and worth professional discussion. |
| 31 – 45 | Moderate — Significant HPD Pattern | Significant histrionic pattern across multiple DSM-5-TR criteria. Consistent with HPD, professional evaluation is recommended. |
| 46 – 60 | High — Strong HPD Indicators | Pervasive histrionic pattern across most criteria. Strongly consistent with HPD. Professional evaluation and therapeutic support are strongly recommended. |
Treatment for Histrionic Personality Disorder
HPD is considered treatment-resistant, with most research reporting limited efficacy and low symptom remission rates (StatPearls, Torrico et al., 2024). This does not mean treatment is futile — it means that realistic expectations focus on improved functioning and relational satisfaction rather than elimination of the personality features. Psychotherapy is the primary modality; no medications are specifically approved for HPD.
Psychodynamic Psychotherapy. The most clinically appropriate approach for HPD given the developmental origins and personality-level nature of the disorder. Psychodynamic work addresses the underlying dynamics driving the attention-seeking pattern — exploring what genuine connection means, what the theatrical performance is protecting against, and how to develop more stable and authentic emotional expression and relationship expectations. The therapeutic relationship itself is a primary vehicle for change.
Cognitive Behavioral Therapy (CBT). Targeting the cognitive patterns that maintain HPD — including the belief that theatrical expression is necessary to be heard, the automatic overestimation of relationship intimacy, and the interpretation of not being the center of attention as abandonment — can produce meaningful behavioral change. CBT is typically more symptom-focused than psychodynamic work and may be more accessible as an initial approach.
Schema Therapy. Addressing the early maladaptive schemas underlying HPD — particularly the schema that one must perform to receive care — may be especially appropriate given the condition’s developmental origins. Schema Therapy’s focus on meeting core emotional needs in more adaptive ways addresses the root motivation driving the histrionic pattern.
Goals of treatment. The Merck Manual (2026) describes treatment goals for HPD as including helping patients develop deeper, more genuine personal relationships; reducing reliance on theatrical emotional expression as the primary mode of communication; and building tolerance for not being the center of attention without the associated distress. Recovery in HPD is measured in relational quality and emotional stability, not in symptom elimination.
Frequently Asked Questions
What is Histrionic Personality Disorder?
Histrionic Personality Disorder (HPD) is a Cluster B personality disorder (DSM-5-TR 301.50 / F60.4) defined as a pervasive pattern of excessive emotionality and attention-seeking, beginning in early adulthood and present in a variety of contexts. Diagnosis requires ≥5 of 8 DSM-5-TR criteria: discomfort when not the center of attention; inappropriate seductive or provocative behavior; rapidly shifting, shallow emotions; use of appearance for attention; impressionistic speech lacking detail; self-dramatization and theatricality; suggestibility; and overestimation of relationship intimacy. Prevalence is approximately 1.84–3% of the general population. Women are diagnosed approximately four times more often than men, though this reflects diagnostic bias as much as real sex differences (APA, 2022).
What is the difference between HPD and narcissistic personality disorder?
Both HPD and NPD involve the need for attention and admiration and are Cluster B disorders — but they are organized around different core needs. HPD is about attention itself: being seen, captivated by, and emotionally connected to. The person with HPD needs to be the focal point. NPD is about admiration of superiority: recognition that they are exceptional, special, and more deserving than others. The narcissist needs to be the most impressive; the histrionic person needs to be the most noticed. Another key distinction: HPD involves emotional expressiveness and lability; NPD typically involves emotional control with rage responses to ego threat. Both disorders can co-occur, and both are part of the Cluster B assessment on the Cluster B Personality Disorder Test.
How is HPD different from borderline personality disorder?
HPD and BPD are the most commonly confused Cluster B disorders because both involve emotional lability, impulsivity, and relationship difficulties. The key distinctions: BPD is organized around fear of abandonment and identity instability — the intense, dysregulated emotions in BPD are genuine responses to perceived abandonment; the emotions in HPD are rapid, shallow, and theatrical rather than deeply felt and dysregulating. BPD involves self-harm, chronic emptiness, and intense identity disturbance that HPD does not. HPD involves the deliberate use of appearance and seductiveness as attention-securing tools and the consistent overestimation of relationship intimacy, which BPD does not specifically involve. Both can be assessed on the BPD Test.
Is HPD more common in women?
HPD is diagnosed approximately four times more often in women than in men. However, researchers and the APA itself note that this likely reflects diagnostic bias as much as genuine sex differences — the DSM-5-TR criteria describe behavioral patterns (seductiveness, theatrical emotional expression, focus on appearance) that are more socially permissible and therefore more visible in women. The same behaviors in men may be labeled differently, attributed to other conditions, or simply not identified as HPD. The actual sex ratio for HPD, if diagnostic bias were accounted for, is believed to be closer to equal than the diagnosed ratio suggests (APA, 2022; Baylor, 2024).
Can someone with HPD have genuine emotional experiences?
Yes — and this is one of the most important misconceptions about HPD to address. The rapidly shifting and shallow emotional expression (Criterion 3) is often interpreted as meaning that people with HPD don’t feel genuine emotions. The clinical picture is more complex: the emotions are real, but they tend to be processed and expressed through a theatrical performance mode that has become habitual, making them appear shallow to observers. The emotions can be genuinely felt in the moment and then genuinely resolved — rapidly — in a way that others find confusing. The challenge is not that the emotions are fake, but that the mode of expression creates a barrier to the authentic, sustained emotional connection that genuine intimacy requires.
What is the long-term course of HPD?
HPD is considered a chronic, lifelong condition with generally low rates of spontaneous remission (StatPearls, Torrico et al., 2024). Unlike some other personality disorders (particularly BPD), there is limited long-term outcome research on HPD. What research exists suggests that the attention-seeking behavior may become less overtly theatrical with age — as social roles and contexts change — but the underlying need for attention and validation typically persists. The most significant long-term consequences of HPD are relational: the pattern of overestimating relationship intimacy, combined with the theatrical emotional expression that others may not take seriously, produces a consistent pattern of shallow, unsatisfying relationships despite the histrionic person’s investment in social connection.
Is HPD the same as being dramatic or extroverted?
No. Dramatic personality and high extraversion are normal personality dimensions that exist on a spectrum. HPD involves a clinically significant, pervasive pattern that causes functional impairment and distress — specifically the inability to tolerate not being the center of attention, the theatrical emotional expression that others perceive as performed, the habitual seductiveness in inappropriate contexts, and the consistent overestimation of intimacy in relationships. The distinction from normal personality variation lies in the pervasiveness, the rigidity, the functional impairment, and the distress — not in the presence of the traits themselves, which exist in everyone to varying degrees.
Related Tests
- Narcissistic Personality Disorder Test — HPD and NPD are the most similar Cluster B disorders; both involve attention-seeking and Cluster B features, through different core needs
- Borderline Personality Disorder Test — BPD and HPD are frequently confused; both involve emotional lability and relationship instability through different mechanisms
- Cluster B Personality Disorder Test — comprehensive assessment across all four Cluster B disorders: HPD, NPD, BPD, and ASPD
- Antisocial Personality Disorder Test — the fourth Cluster B disorder; ASPD and HPD co-occur in some presentations
- Dark Triad Test — measures narcissism, Machiavellianism, and psychopathy as overlapping dark personality dimensions relevant to HPD presentations
- Bipolar Test — bipolar disorder’s mood episodes can superficially resemble HPD’s emotional expressiveness; important differential
- Dependent Personality Disorder Test — DPD and HPD both involve high dependency on others’ approval; they co-occur and share developmental roots
- Clinical Depression Test — people with HPD often become depressed when they are not the center of attention; comorbid depression needs separate assessment
- Anxiety Test — anxiety disorders are among the most common HPD comorbidities
- Full Personality Disorder Test Hub — all ten DSM-5-TR personality disorder types across Clusters A, B, and C
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Histrionic Personality Disorder 301.50 (F60.4), pp. 757–760. psychiatry.org
- Torrico, T.J., French, J.H., & Aslam, S.P. (2024). Histrionic Personality Disorder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Updated June 20, 2024. [Chronic; treatment-resistant; low remission] statpearls.com
- Merck Manual Professional Edition. (2026). Histrionic Personality Disorder. [Criteria; prevalence; treatment goals] merckmanuals.com
- Zimmerman, M., Rothschild, L., & Chelminski, I. (2005). The prevalence of DSM-IV personality disorders in psychiatric outpatients. American Journal of Psychiatry, 162(10), 1911–1918. [1.84% general population] doi.org
- Novais, F., Araújo, A., & Godinho, P. (2015). Historical roots of histrionic personality disorder. Frontiers in Psychology, 6, 1463. [Etymology; Charcot; Freud and Breuer] doi.org
- Palm, M. (2024). Histrionic Personality Disorder. In: Understanding Psychological Disorders. Baylor University Open Textbook. [2–3% prevalence; women 4x more diagnosed] openbooks.library.baylor.edu
- EBSCO Research Starters. (2025). Histrionic Personality Disorder (HPD). [<2% general population] ebsco.com
- Wikipedia. (2025). Histrionic personality disorder. en.wikipedia.org