
The fear arrives before there’s evidence for it. Someone takes longer than usual to reply and the dread is immediate — complete, physical, as certain as any real signal of danger. The person you loved yesterday becomes, with a comment or a distance, the person you cannot bear. And underneath both of these — the love and the rage, the connection and the panic — there is the recurring question of who you actually are when none of that is happening.
Borderline Personality Disorder is one of the most misrepresented and misunderstood conditions in mental health — stigmatized in clinical settings, mischaracterized in popular culture, and yet experienced by the people who have it as the most painful and destabilizing of inner states. It is not a character flaw. It is not manipulation. It is not untreatable. It is a recognized, well-researched psychiatric condition with effective treatments that produce significant and lasting improvement.
This free Borderline Personality Disorder Test (BPD) covers all 9 DSM-5-TR diagnostic criteria for Borderline Personality Disorder (APA, 2022). 18 questions. Instant, private results.
If you are experiencing thoughts of self-harm or suicide, please reach out now.
📞 988 Suicide & Crisis Lifeline — Call or text 988 (United States, 24/7)
🌐 Crisis Text Line: Text HOME to 741741
You do not have to be in immediate danger to reach out. If the emotional pain feels unmanageable right now, these lines are for you.
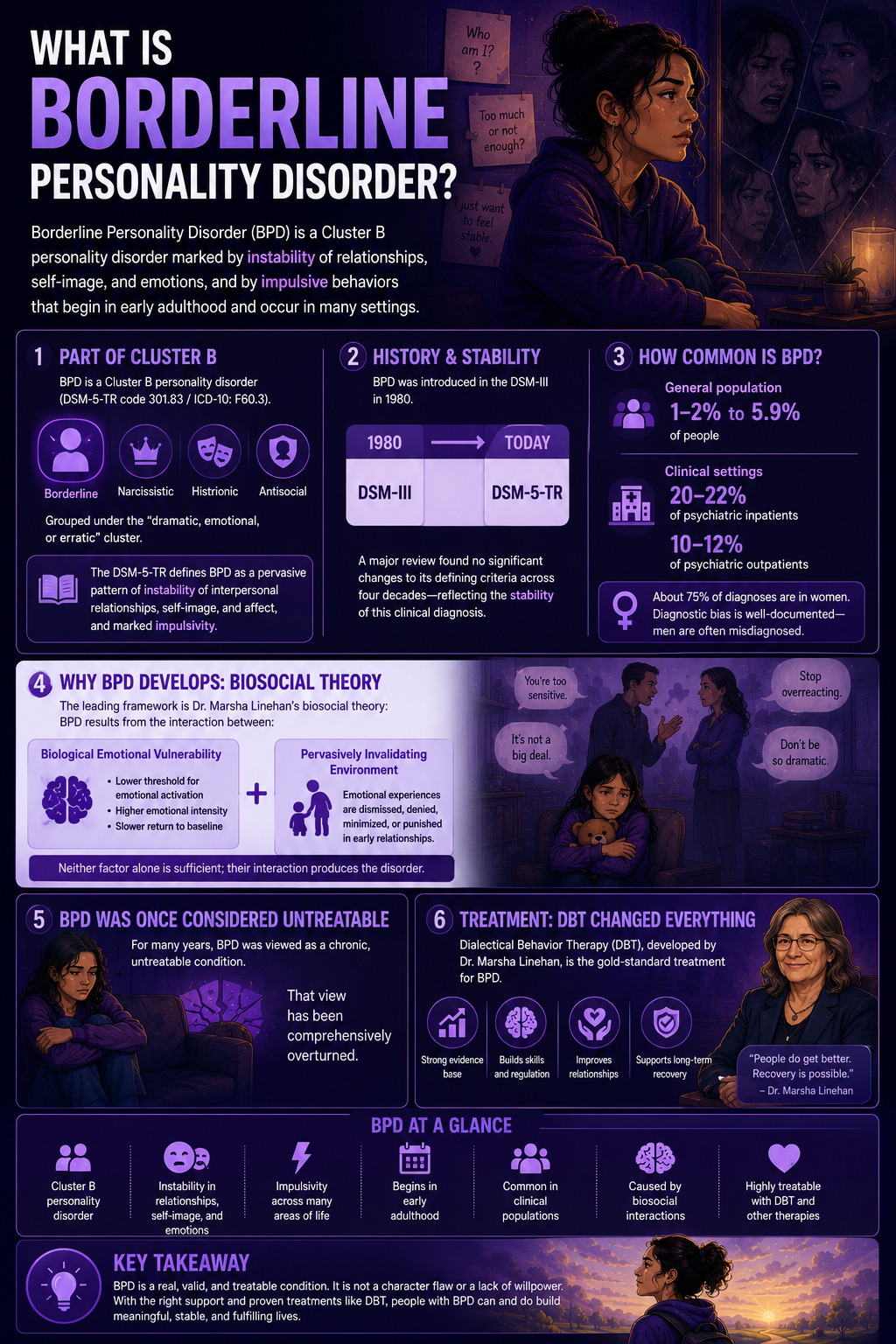
What Is Borderline Personality Disorder?
Borderline Personality Disorder (BPD) is a Cluster B personality disorder (DSM-5-TR code 301.83 / ICD-10: F60.3) — grouped alongside Narcissistic, Histrionic, and Antisocial Personality Disorders under the “dramatic, emotional, or erratic” cluster. The DSM-5-TR defines BPD as a pervasive pattern of instability of interpersonal relationships, self-image, and affect, and marked impulsivity, beginning in early adulthood and present in a variety of contexts (APA, 2022).
BPD was introduced as a formal diagnosis in the DSM-III in 1980. A landmark comprehensive review by Leichsenring and colleagues (World Psychiatry, 2024) documented that from the DSM-III to the DSM-5-TR, no major changes have occurred in its defining criteria — reflecting the stability of the clinical construct over four decades of research.
Prevalence estimates range from 1–2% of the general population (Medscape, 2025; Martín-Vázquez, Archives of Depression and Anxiety, 2025) to 5.9% in some broader studies (Vanwoerden et al., 2019). In clinical settings, prevalence is substantially higher: approximately 20–22% of psychiatric inpatient populations and 10–12% of psychiatric outpatient populations meet BPD criteria (eCare Behavioral Health Institute, 2025). Approximately 75% of BPD diagnoses are in women — though diagnostic bias is well-documented, with men more likely to be misdiagnosed with depression, PTSD, or antisocial personality disorder when the underlying condition is BPD (eCare, 2025; Broadbear et al., 2025, cited in ScienceDirect).
The leading etiological framework for BPD is Dr. Marsha Linehan’s biosocial theory: BPD results from the interaction between a biological emotional vulnerability — a lower threshold for emotional activation, higher emotional intensity, and slower return to baseline — and a pervasively invalidating environment — an early relational context in which the child’s emotional experiences were consistently dismissed, denied, minimized, or punished (Linehan et al., cited in Medscape, 2025; ScienceDirect, 2025). Neither factor alone is sufficient; their interaction produces the disorder.
BPD was historically considered untreatable. This view has been comprehensively overturned — most notably by the development of Dialectical Behavior Therapy (DBT) by Dr. Marsha Linehan, which has become the gold-standard treatment for BPD with robust evidence for significant and lasting improvement (ScienceDirect, 2025; Leichsenring et al., World Psychiatry, 2024).
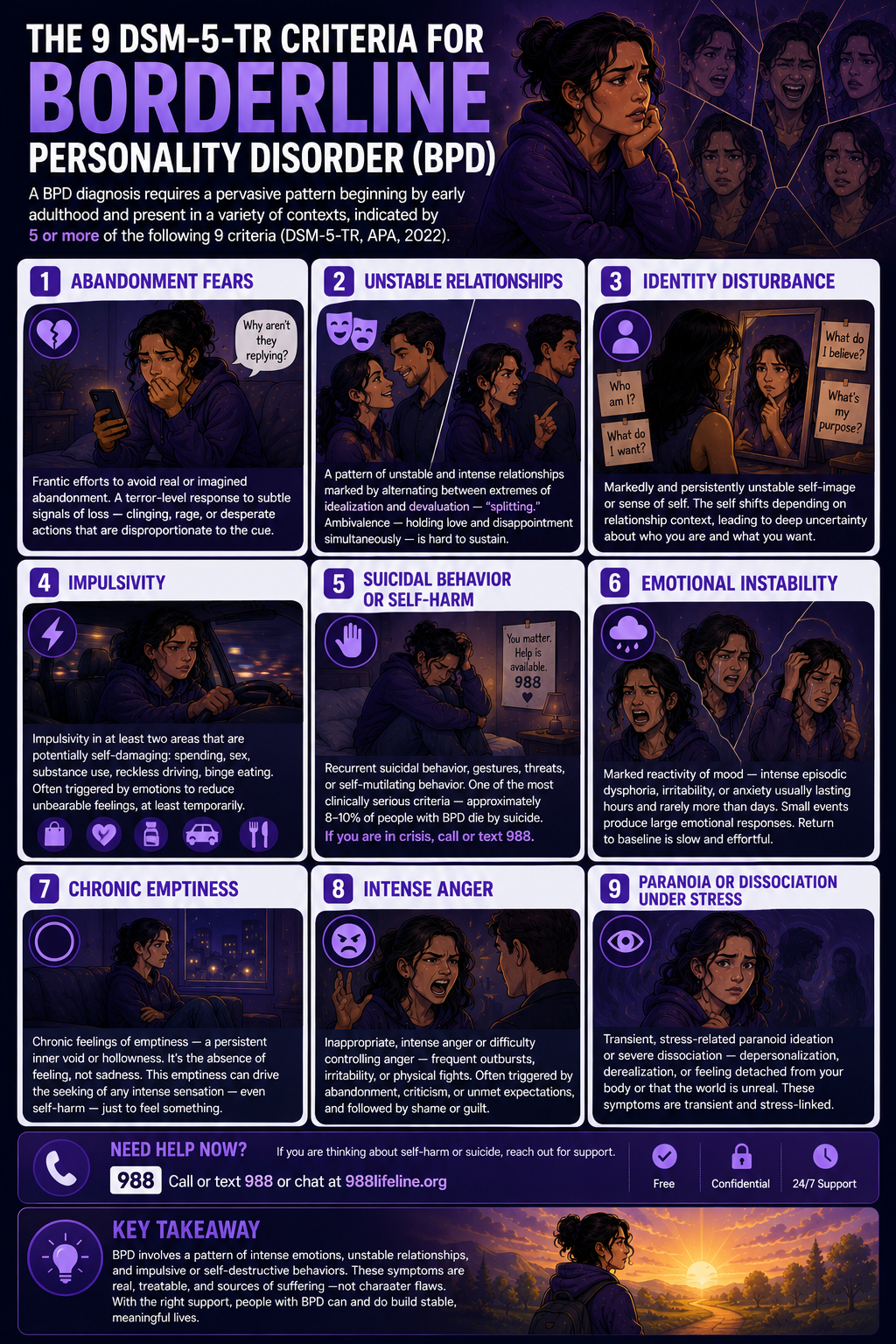
The 9 DSM-5-TR Criteria for BPD
A BPD diagnosis requires a pervasive pattern beginning by early adulthood and present in a variety of contexts, indicated by ≥5 of the following 9 criteria (APA, 2022):
Abandonment fears
Frantic efforts to avoid real or imagined abandonment. Unlike ordinary discomfort at the prospect of loss, this is a terror-level response activated by perceived signals of abandonment that may be subtle, ambiguous, or entirely imagined — a delayed text message, a shift in tone, someone seeming slightly distant. The response — clinging, rage, desperate action — is disproportionate to the actual signal.
Unstable relationships
A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation — “splitting.” The person you put on a pedestal and the person who has completely let you down are the same person, perceived through completely different lenses depending on the current emotional state. True ambivalence — holding love and disappointment simultaneously — is difficult to sustain.
Identity disturbance
Markedly and persistently unstable self-image or sense of self. Not the ordinary variation in self-perception that everyone experiences, but a deeper uncertainty: who am I when I’m not with this person? What do I actually want? What do I actually believe? The self shifts substantially depending on the relationship context, leaving a sense of not having a stable core.
Impulsivity
Impulsivity in at least two areas that are potentially self-damaging: spending, sex, substance use, reckless driving, binge eating. The impulsivity is often triggered by emotional states and serves a regulatory function — the action reduces the intensity of an unbearable feeling, at least temporarily.
Suicidal behavior or self-harm
Recurrent suicidal behavior, gestures, threats, or self-mutilating behavior. This is one of the most clinically serious BPD criteria and one of the most important reasons that BPD requires careful, professional evaluation. Approximately 8–10% of people with BPD die by suicide. If you are experiencing self-harm thoughts, please reach out to 988 (call or text) before continuing.
Emotional instability
Marked reactivity of mood — intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days. The emotional reactions are intense but brief — unlike the sustained mood episodes of bipolar disorder. Small events produce large emotional responses. The return to baseline is slow and effortful.
Chronic emptiness
Chronic feelings of emptiness — a persistent inner void or hollowness that many people with BPD describe as one of the most painful and hardest-to-communicate features of the condition. The emptiness is not sadness; it is the absence of feeling, a flatness that can trigger the seeking of any intense sensation — including self-harm — as a way of feeling something.
Intense anger
Inappropriate, intense anger or difficulty controlling anger — frequent temper outbursts, constant irritability, recurrent physical fights — often followed by shame or guilt. The anger is often triggered by perceived abandonment, criticism, or failure to meet expectations, and its intensity can be disproportionate to the trigger, damaging relationships.
Paranoia or dissociation under stress
Transient, stress-related paranoid ideation or severe dissociative symptoms. When under significant interpersonal stress, the person with BPD may briefly experience paranoid thoughts about others’ intentions or dissociative symptoms — depersonalization, derealization, feeling detached from their body or that the world is unreal. These experiences are transient and stress-linked, distinguishing them from the persistent paranoia of psychotic disorders.
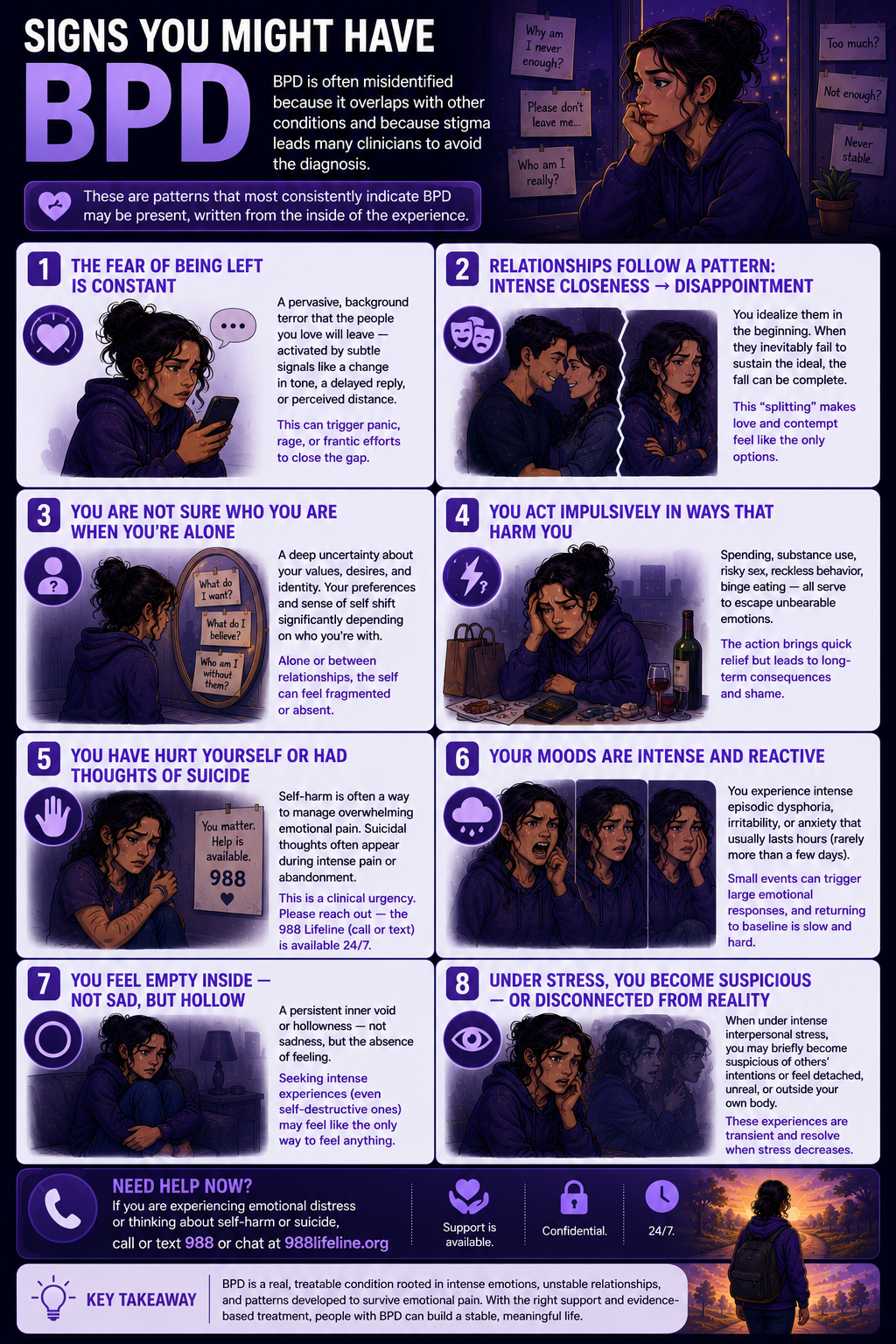
Signs You Might Have BPD
BPD is among the most commonly misidentified conditions — both because its presentation overlaps with several other conditions and because the stigma around the diagnosis leads many clinicians to avoid it. These are the patterns that most consistently indicate BPD may be present, written from the inside of the experience rather than from the outside.
The fear of being left is constant — and it activates at signals most people wouldn’t register. This is not ordinary attachment anxiety. It is a pervasive, background terror that the people you love will leave — and a hypersensitivity to any signal that this might be happening. A slight change in tone, a delayed reply, a perceived distance that others might not even notice can activate the full abandonment response: panic, rage, or frantic efforts to close the gap before the loss becomes real.
Your most important relationships follow a pattern — intense closeness followed by disappointment and sometimes contempt. The idealization is genuine: in the early stages of a close relationship, the person feels exactly what you’ve always needed. The devaluation is also genuine: when the person inevitably fails to sustain the idealization — by being human, by being imperfect, by having needs of their own — the fall can be complete. The technical term is splitting. The lived experience is loving someone fully and then not being able to access that love at all.
You are not sure who you are when you’re alone. The identity disturbance of BPD is not self-consciousness or lack of confidence — it is a deeper uncertainty about what you actually value, what you actually want, and who you actually are. Your preferences, opinions, and sense of self shift significantly depending on who you’re with. When you’re alone, or between relationships, the self can feel fragmented or absent.
You act impulsively in ways that harm you — and the impulse is often driven by an emotion you’re trying to escape. Spending, substance use, risky sex, reckless behavior, binge eating — these are the specific areas the DSM-5-TR identifies, and they share a common function: they reduce the intensity of an unbearable emotional state quickly. The action is not planned; it is a response to pain. It works in the short term and costs in the longer term, producing shame that adds to the emotional dysregulation it was meant to relieve.
You have hurt yourself or had thoughts of suicide as a response to emotional pain. Self-harm in BPD typically functions as an emotion regulation strategy — a way of converting an unbearable internal experience into a manageable physical one. Suicidal thoughts often appear during moments of intense emotional pain or abandonment. Both represent a clinical urgency that makes professional evaluation and support essential. If this describes you, please reach out — the 988 Lifeline (call or text) is available 24/7.
Your moods are intense and reactive — and small events produce large emotional responses. The emotional reactivity of BPD is not drama or exaggeration — it is the biological emotional vulnerability that Linehan’s biosocial theory describes: a lower activation threshold, higher emotional intensity, and a slower return to baseline. An emotional state that most people would experience as a mild annoyance can arrive as a full emotional crisis. The intensity is real. The difficulty returning to baseline is real.
You feel empty inside — not sad, but hollow. The chronic emptiness of BPD is one of its least discussed and most painful features. It is not depression — it lacks the quality of sadness, grief, or hopelessness. It is more like the absence of anything — a hollow flatness that can make seeking intense experiences (including self-destructive ones) feel like the only alternative to feeling nothing at all.
Under stress, you become suspicious of others’ intentions — or feel disconnected from yourself or reality. The paranoia and dissociation of Criterion 9 are transient, stress-linked, and interpersonally triggered. When the threat of abandonment or interpersonal failure is intense, the perception of others’ intentions may become suspicious (“they are doing this on purpose”), or the sense of self may fragment into a dissociative state — feeling detached, unreal, or outside your own body. These experiences resolve with the reduction of stress.
Quiet BPD — The Presentation Most People Don’t Recognize
“Quiet BPD” (also called “high-functioning BPD”) is a colloquial term for a BPD presentation in which the emotional intensity is directed inward rather than outward. Where the classic BPD presentation involves externally visible emotional reactivity — rage, impulsive behavior, dramatic relationship crises — quiet BPD involves the same internal experience (abandonment terror, emotional dysregulation, identity disturbance, chronic emptiness) expressed through withdrawal, self-harm, internal splitting, and carefully maintained external composure.
People with quiet BPD often appear high-functioning from the outside while experiencing severe internal distress. They are less likely to be identified or diagnosed because the explosive outward presentations that clinicians associate with BPD are absent. The same nine DSM-5-TR criteria apply — the difference is in direction of expression, not in the underlying disorder.
If the patterns described in this BPD test resonate internally — the abandonment fears, the splitting, the chronic emptiness, the identity instability — but you don’t act them out in ways others would notice, quiet BPD may be more accurate than the clinical picture you’ve previously received. A therapist experienced with BPD can assess this distinction properly.
BPD vs C-PTSD vs Bipolar Disorder vs NPD — The Critical Differentials
| Feature | BPD | C-PTSD | Bipolar II | Narcissistic PD (NPD) |
|---|---|---|---|---|
| Core driver | Fear of abandonment + identity instability | Chronic trauma response + self-organization disturbances | Episodic mood states (hypomania + MDE) | Need for admiration + grandiosity + entitlement |
| Mood pattern | Reactive, brief mood shifts triggered by interpersonal events — hours, not days | Affect dysregulation rooted in trauma responses; more stable between triggers | Sustained mood episodes (days to weeks) not primarily triggered by interpersonal events | Generally controlled; rage when ego threatened; not characterized by mood lability |
| Self-concept | Unstable, fragmenting, identity-uncertain; chronic emptiness | Persistently negative self-concept — damaged, worthless, permanently harmed | Stable between episodes; self-concept not a defining feature | Inflated but fragile; grandiosity protects against underlying shame |
| Relationships | Intense splitting — idealization then devaluation driven by abandonment fear | Relational disturbances rooted in trauma — distrust, difficulty with intimacy | Affected by mood episodes; not characterized by splitting or abandonment dynamics specifically | Exploitative; idealize then devalue based on whether person affirms or challenges grandiosity |
| Self-harm / suicide risk | High — recurrent self-harm and suicidality are DSM criterion 5; ~8–10% die by suicide | Elevated — trauma history; may use self-harm for affect regulation similarly to BPD | Elevated — particularly during depressive and mixed episodes | Lower than Cluster B average; narcissistic injury may produce suicidality |
| Primary treatment | DBT (gold standard); MBT; TFP — all personality-focused | Phase-based trauma therapy — stabilization before processing | Mood stabilizers (lithium, lamotrigine); IPSRT | Schema Therapy; TFP — long-term personality work |
| PsyMed test | This test | PTSD Test | Bipolar Test | NPD Test |
The BPD/C-PTSD differential is particularly important — and particularly contested. Both involve emotional dysregulation, relational instability, self-harm, and a history of trauma. Many clinicians argue that what the DSM-5-TR classifies as BPD in people with significant childhood trauma histories is better understood as C-PTSD (ICD-11). Both diagnoses can be accurate simultaneously, and the treatment overlap (particularly stabilization-focused approaches) is significant. The PTSD Test is worth completing alongside this one.
What Causes Borderline Personality Disorder?
BPD etiology is best understood through Linehan’s biosocial theory — the most empirically supported and clinically influential etiological framework.
Biosocial theory (Linehan). BPD develops from the interaction of two factors: biological emotional vulnerability (a lower threshold for emotional activation, higher emotional intensity, and slower return to emotional baseline — present from birth as a temperamental feature) and a pervasively invalidating environment (an early relational context in which the child’s emotional experiences were consistently dismissed, punished, minimized, or denied as invalid). Neither factor alone is sufficient — but the combination, particularly in critical developmental periods, produces the emotional dysregulation, identity instability, and relational patterns that define BPD (Medscape, 2025; ScienceDirect, 2025).
Trauma and attachment. A significant proportion of people with BPD have histories of childhood abuse, neglect, or attachment disruption. The invalidating environment of the biosocial model frequently includes active abuse or neglect, though it also encompasses subtler forms of chronic emotional dismissal. Early attachment disruption shapes the relational templates that produce the abandonment fears and splitting of BPD.
Neurobiological factors. Neuroimaging research has identified structural and functional differences in the amygdala (hyperreactivity), prefrontal cortex (reduced regulatory function), and anterior cingulate cortex in BPD — consistent with the biosocial model’s emphasis on biological emotional reactivity and impaired affect regulation (Leichsenring et al., World Psychiatry, 2024).
Genetic factors. BPD shows significant heritability — estimated at 40–60% in twin studies. The heritable component likely reflects the biological emotional vulnerability dimension of the biosocial model.
Comorbidities. BPD has very high comorbidity rates. Approximately 85% of people with BPD meet criteria for at least one other Axis I disorder (Leichsenring et al., 2024). The most common comorbidities are major depressive disorder, PTSD, anxiety disorders, and substance use disorders (Martín-Vázquez, 2025). The bipolar disorder differential is particularly important given shared features of mood reactivity and impulsivity. ADHD frequently co-occurs with BPD and shares impulsivity and emotional dysregulation.
How This Borderline Personality Disorder Test Works
This BPD Test covers all 9 DSM-5-TR criteria for Borderline Personality Disorder across 18 questions — abandonment fears, splitting, identity disturbance, impulsivity, self-harm and suicidality, emotional reactivity, chronic emptiness, anger dysregulation, and stress-related paranoia or dissociation.
The test can be completed for yourself or answered with someone in your life in mind. Answer based on your consistent experience over the past several months — the recurring pattern, not specific crisis moments or best periods.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–72. This is a screening tool. Only a qualified mental health professional can diagnose BPD — a clinical interview, collateral information, and functional assessment are required.
Understanding Your BPD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 18 | Low — Few BPD Indicators | Few significant BPD patterns present. Emotional intensity and relationship difficulties may be present within the normal range without a pattern consistent with BPD. |
| 19 – 36 | Mild — Some BPD Patterns Present | Some BPD-related patterns present across one or more criterion areas. May reflect subthreshold BPD or early-stage features. Warrants professional discussion. |
| 37 – 54 | Moderate — Significant BPD Pattern | Significant BPD features across multiple criteria. Consistent with BPD; professional evaluation is strongly recommended. If self-harm thoughts are present, please contact 988. |
| 55 – 72 | High — Strong BPD Indicators | Pervasive BPD pattern across most criteria. Professional evaluation and DBT-specialized treatment are urgently recommended. If you are in crisis, please call or text 988 now. |
Treatment for Borderline Personality Disorder
BPD is highly treatable. The historical view of BPD as untreatable has been comprehensively overturned by decades of controlled treatment research (Leichsenring et al., World Psychiatry, 2024).
Dialectical Behavior Therapy (DBT). The gold-standard treatment for BPD was developed by Dr. Marsha Linehan at the University of Washington. DBT combines individual therapy, skills training group, phone coaching, and a therapist consultation team. The four DBT skill modules — Mindfulness (grounding in the present moment), Distress Tolerance (managing crisis without making it worse), Emotion Regulation (understanding and modulating emotional states), and Interpersonal Effectiveness (navigating relationships skillfully) — directly address the core BPD features. DBT produces significant reductions in suicidality, self-harm, emotional dysregulation, and interpersonal dysfunction in the majority of completers.
Mentalization-Based Therapy (MBT). Developed by Dr. Peter Fonagy and Anthony Bateman, MBT targets the failure in mentalizing — the capacity to understand one’s own and others’ mental states — that underlies many BPD interpersonal difficulties. MBT has strong evidence from randomized controlled trials, including long-term follow-up data.
Transference-Focused Psychotherapy (TFP). Developed by Dr. Otto Kernberg, TFP uses the therapeutic relationship to identify and modify the split object representations — the all-good and all-bad relational patterns — that drive BPD relationship dynamics. Evidence supported in controlled trials.
Pharmacotherapy. No medications are specifically FDA-approved for BPD, but medications are used to target specific symptom domains — mood stabilizers or antipsychotics for emotional dysregulation and impulsivity, SSRIs for depression and anxiety. Medication is typically adjunctive to psychotherapy rather than primary.
Frequently Asked Questions
What is Borderline Personality Disorder?
Borderline Personality Disorder (BPD) is a Cluster B personality disorder (DSM-5-TR 301.83 / F60.3) defined as a pervasive pattern of instability of interpersonal relationships, self-image, and affect, and marked impulsivity, beginning by early adulthood. Diagnosis requires ≥5 of 9 criteria: abandonment fears, unstable relationships with splitting, identity disturbance, self-damaging impulsivity, suicidal or self-harm behavior, emotional instability, chronic emptiness, inappropriate intense anger, and stress-related paranoia or dissociation. Prevalence is 1–2% of the general population; 20–22% in psychiatric inpatient settings. DBT is the gold-standard evidence-based treatment (ScienceDirect, 2025; APA, 2022).
What is the difference between BPD and bipolar disorder?
BPD and bipolar disorder are among the most commonly confused conditions. The critical distinction is in the mood pattern: BPD involves brief, intense emotional reactions (hours, not days) that are triggered by interpersonal events — specifically abandonment fears, perceived rejection, or relational conflict. Bipolar disorder involves sustained mood episodes (days to weeks of mania/hypomania or depression) that occur largely independently of interpersonal triggers and represent a categorical shift from the person’s baseline. The identity instability, splitting, chronic emptiness, and abandonment fears that define BPD are not features of bipolar disorder. Both can co-occur. Complete the Bipolar Test if sustained mood episodes are also present.
What is quiet BPD?
“Quiet BPD” or “high-functioning BPD” describes a BPD presentation where emotional intensity is directed inward rather than outward. All nine DSM-5-TR criteria can be present, but the externally visible behavioral manifestations — rage, dramatic relational crises, visible impulsivity — are absent or contained. The internal experience is equally intense: the abandonment fears, splitting, emptiness, and identity instability are fully present. People with quiet BPD are less likely to be diagnosed because the presentations clinicians expect from BPD are absent. This is one of the primary forms of diagnostic underidentification, particularly in women who have learned to suppress rather than express emotional reactivity.
Is BPD treatable?
Yes — BPD is highly treatable, and the historical view of BPD as untreatable has been comprehensively overturned. Dialectical Behavior Therapy (DBT), developed by Dr. Marsha Linehan, has become the gold-standard treatment with robust evidence for significant improvements in suicidality, self-harm, emotional dysregulation, and interpersonal function (Leichsenring et al., World Psychiatry, 2024; ScienceDirect, 2025). Mentalization-Based Therapy (MBT) and Transference-Focused Psychotherapy (TFP) are also evidence-supported. The prognosis for BPD with appropriate, specialized treatment is substantially better than for many other personality disorders.
What is the relationship between BPD and trauma?
A significant proportion of people with BPD have histories of childhood abuse, neglect, or attachment disruption. Linehan’s biosocial theory specifically identifies the “pervasively invalidating environment” — which frequently involves active trauma — as one of the two factors in BPD etiology. The overlap between BPD and C-PTSD (ICD-11) is substantial: both involve emotional dysregulation, relational disturbances, negative self-concept, and self-harm, and both often share a trauma history. The BPD/C-PTSD differential is clinically important but contested — many researchers argue that trauma-based presentations currently diagnosed as BPD are better understood as C-PTSD. Complete the PTSD Test alongside this one if trauma history is relevant.
Can men have BPD?
Yes — BPD occurs in men, but is significantly underdiagnosed. The approximately 75% female diagnosis rate reflects diagnostic bias as much as real sex differences. Men with BPD are more likely to be misdiagnosed with depression, PTSD, antisocial personality disorder, or substance use disorder when the underlying condition is BPD — because the criteria were developed and validated primarily in female samples, and because gendered expectations about emotional expression mean that the same behaviors are interpreted differently in men (eCare Behavioral Health Institute, 2025; Broadbear et al., 2025). Men with BPD may present with more pronounced externalizing features (substance use, aggression) and less prominent internalizing features (self-harm, emptiness) than women, though both patterns occur in both sexes.
What should I do if I think I have BPD?
The most important step is seeking a proper clinical evaluation from a mental health professional experienced with personality disorders. BPD is best assessed through a clinical interview that covers developmental history, current symptom profile, and functional impact — not through self-report alone. When you reach out, you can say: “I believe I may have BPD and I’d like a proper evaluation.” Specifically look for therapists and psychiatrists with DBT training or experience treating BPD — the treatment specialization matters significantly for outcomes. NAMI (National Alliance on Mental Illness, nami.org) and the Treatment and Research Advancements Association for Personality Disorders (TARA4BPD) can help locate specialized providers.
Related Tests
- PTSD Test — the BPD/C-PTSD differential is one of the most important in clinical practice; trauma history and BPD frequently co-occur; complete both
- Bipolar Test — bipolar disorder is the most commonly confused condition with BPD; both involve mood variability and impulsivity through different mechanisms
- Narcissistic Personality Disorder Test — both Cluster B; NPD and BPD share idealization-devaluation patterns but through different core dynamics
- Cluster B Personality Disorder Test — comprehensive assessment across all four Cluster B disorders
- Covert Narcissism Test — covert NPD and BPD share shame sensitivity, relational instability, and splitting; important to distinguish
- Clinical Depression Test — MDD is the most common BPD comorbidity; approximately 85% of people with BPD have at least one comorbid Axis I disorder
- Anxiety Test — anxiety disorders are among the most common BPD comorbidities
- ADHD Test — ADHD and BPD share impulsivity and emotional dysregulation; they frequently co-occur and can be difficult to distinguish
- Dissociation Test — dissociation is a BPD criterion (Criterion 9) and is common in the context of childhood trauma that often precedes BPD
- Suicidal Ideation Test — BPD carries an approximately 8–10% completed suicide rate; please assess suicidal ideation alongside BPD features
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Borderline Personality Disorder 301.83 (F60.3), pp. 751–756. psychiatry.org
- Leichsenring, F., Fonagy, P., Heim, N., Kernberg, O.F., et al. (2024). Borderline personality disorder: a comprehensive review of diagnosis and clinical presentation, etiology, treatment, and current controversies. World Psychiatry, 23(1), 4–25. [DSM-III 1980; no major changes to DSM-5; DBT evidence; neurobiology] pmc.ncbi.nlm.nih.gov
- Martín-Vázquez, M.J. (2025). Evidence Psychotherapy Options for Borderline Personality Disorders. Archives of Depression and Anxiety, 11(2), 008–015. [1–2%; PTSD comorbidity; significant suicide rate] dx.doi.org
- ScienceDirect. (2025). Understanding borderline personality disorder: Clinical features, neurobiological insights, and therapeutic strategies. [Linehan biosocial theory; DBT gold standard; diagnostic bias Broadbear et al. 2025] sciencedirect.com
- eCare Behavioral Health Institute. (2025). 20 Borderline Personality Disorder Statistics for 2025. [20-22% inpatient; 10-12% outpatient; 75% female; diagnostic bias] ecarebehavioralinstitute.com
- Medscape. (2025). Borderline Personality Disorder: Practice Essentials, Background, Pathophysiology. [1–2% prevalence; biosocial theory; Linehan] emedicine.medscape.com
- MH Stats. (2026). Borderline Personality Disorder Statistics 2026. [Prevalence; COVID-19 impact; treatment dropout; societal costs] mhstats.org
- Wikipedia. (2025). Borderline personality disorder. en.wikipedia.org