Something feels off. Maybe it’s thoughts that don’t connect the way they used to. Experiences that others don’t seem to share. A growing sense that the world around you is sending signals meant specifically for you — or that certain sounds or voices are arriving from somewhere no one else can access. If something like this brought you here, taking it seriously is the right instinct.
Schizophrenia gets misrepresented constantly. It is not multiple personalities — that’s a different condition entirely, and the confusion has done real damage to how people understand this illness. Most people with schizophrenia are not dangerous. Many hold jobs, maintain relationships, and lead full lives — especially with appropriate treatment. What they navigate is something quieter and stranger than the dramatic portrayals suggest: thoughts that fragment, emotions that flatten, a world that sometimes seems to carry meanings others cannot see.
This free Schizophrenia Test screens for the core symptoms of schizophrenia and psychosis using DSM-5-TR diagnostic criteria (APA, 2022). 15 questions. Instant, private results. It is not a diagnostic tool — only a psychiatrist can diagnose schizophrenia — but it can help you understand whether professional evaluation is the right next step.
If you are in crisis right now, please reach out before taking this test.
📞 988 Suicide & Crisis Lifeline — Call or text 988 (United States, 24/7)
🌐 International: IASP Crisis Centers Directory
If you are experiencing command hallucinations or feel unsafe, please go to your nearest emergency room or call emergency services.
What Is Schizophrenia?
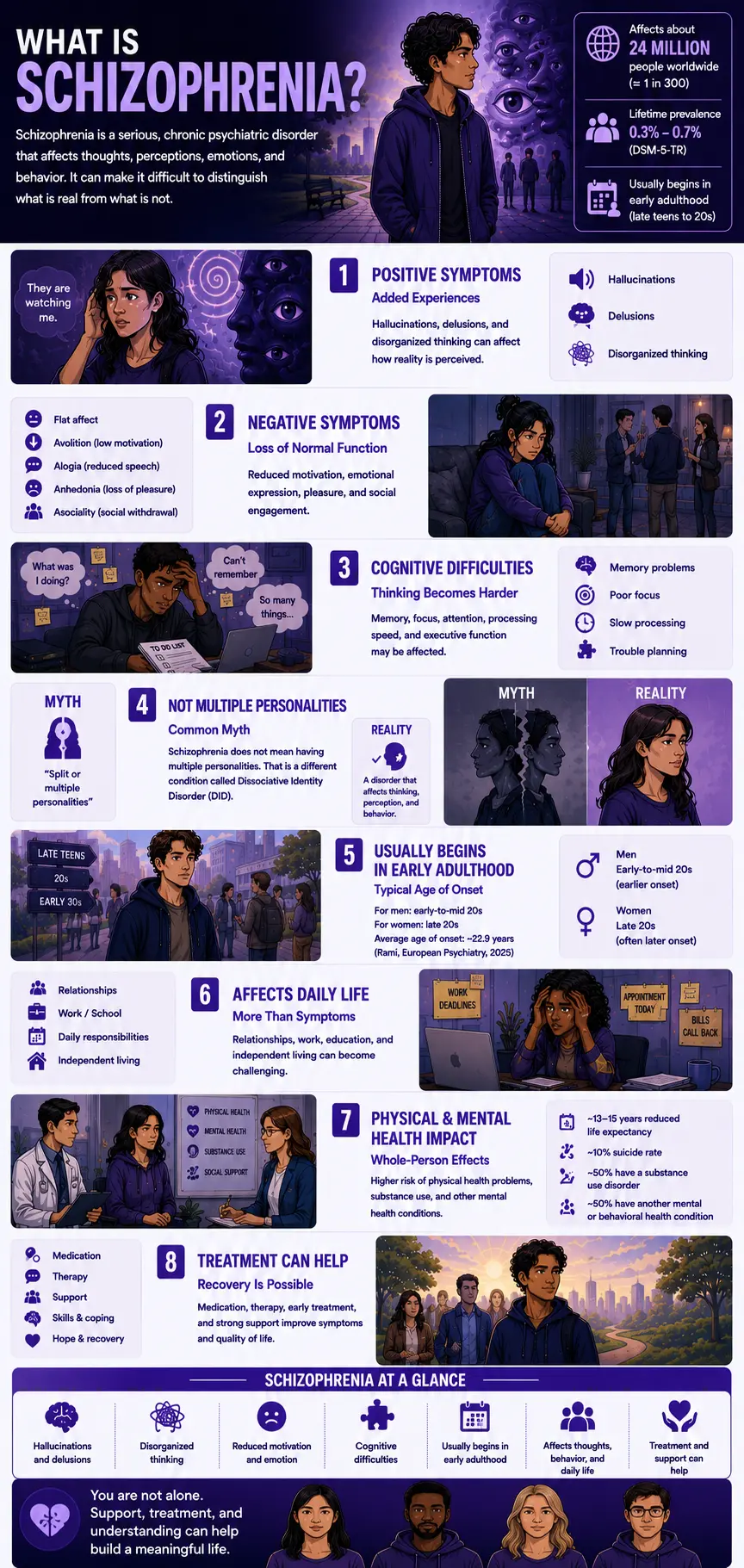
Schizophrenia is a serious, chronic psychiatric disorder classified under Schizophrenia Spectrum and Other Psychotic Disorders in the DSM-5-TR (APA, 2022; code 295.90 / F20.9). It is characterized by disturbances in thought, perception, emotion, and behavior — specifically involving breaks from shared reality through positive symptoms (hallucinations, delusions, disorganized thinking), loss of normal functioning through negative symptoms (flat affect, avolition, alogia, anhedonia, asociality), and impairments in cognition that affect memory, processing speed, and executive function.
The term “schizophrenia” was coined by Swiss psychiatrist Eugen Bleuler in 1911 from the Greek for “split mind” — referring to the fragmentation of mental processes, not to split or multiple personalities. The multiple personality confusion has persisted for over a century and is clinically incorrect; Dissociative Identity Disorder is an entirely different condition.
Schizophrenia affects approximately 24 million people globally — about 1 in 300 (0.32%) worldwide, and 1 in 222 (0.45%) among adults (WHO, 2022; TherapyRoute, 2025). In the United States, prevalence is estimated at 0.25–0.64% (TherapyRoute, 2025). The DSM-5-TR places lifetime prevalence at 0.3–0.7% (APA, 2022). StatPearls (Hany & Rizvi, 2024) cites approximately 1% of the global population. By any measure, schizophrenia is less common than depression or anxiety — but its per-person impact is profound. It is one of the top 15 leading causes of disability worldwide (TherapyRoute, 2025).
Onset is almost always in early adulthood. For men, the first psychotic episode typically occurs in the early-to-mid 20s; for women, in the late 20s (Medscape; DSM-5-TR). A 2025 study (Rami, European Psychiatry) found an average age of onset of 22.91 years across 150 patients. Males tend to be diagnosed earlier and often have a more difficult early course, possibly because estrogen has an antidopaminergic effect that delays onset in women (Medscape, 2025). Overall lifetime prevalence is roughly equal between sexes.
Schizophrenia significantly affects life expectancy: people with schizophrenia have a life expectancy reduced by an estimated 13–15 years compared to the general population, due to increased rates of physical health problems, reduced access to healthcare, and a suicide rate of approximately 10% (StatPearls, Hany & Rizvi, 2024). Approximately 50% of people with schizophrenia have a lifetime history of substance use disorder, and approximately 50% have at least one co-occurring mental or behavioral health condition (DSM-5-TR; TherapyRoute, 2025).
DSM-5-TR Diagnostic Criteria for Schizophrenia
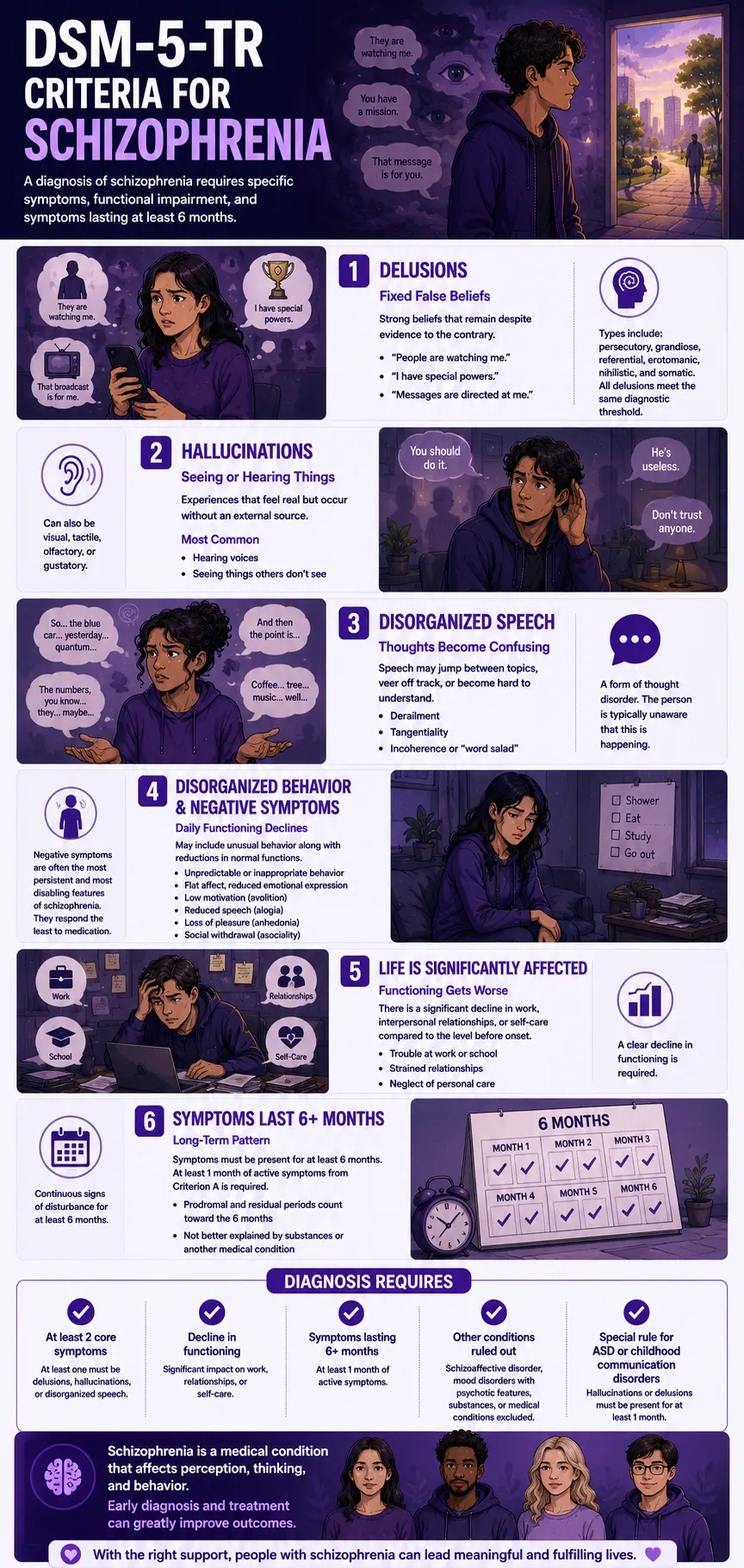
A diagnosis of schizophrenia requires all of the following (APA, 2022):
Criterion A — At least 2 of 5 symptoms, present for ≥1 month. At least one must be from the first three.
1. Delusions — Fixed, false beliefs that are resistant to evidence and inconsistent with the person’s cultural background. Common subtypes include persecutory (“they are watching or following me”), grandiose (“I have a special mission or power”), referential (“that broadcast is sending messages specifically for me”), erotomanic, nihilistic, and somatic. The DSM-5 removed the previous special status of “bizarre” delusions — all delusions now meet the same diagnostic threshold.
2. Hallucinations — Sensory experiences without an external stimulus — vivid, clear, and with the full force of normal perception. Most commonly auditory: voices that comment on behavior, argue with each other, or issue commands. Can also be visual, tactile, olfactory, or gustatory. Hearing one’s name called at the threshold is common in the general population; persistent, clear voices conversing in the third person about the person are qualitatively different.
3. Disorganized speech — Formal thought disorder made manifest in speech. Includes frequent derailment (jumping between unrelated topics), tangentiality (responses that never quite arrive at the point), and in severe cases, incoherence or “word salad” (words assembled without meaningful grammatical or semantic structure). The person is typically unaware that this is occurring.
4. Grossly disorganized or catatonic behavior — Unpredictable agitation, silliness, or behavioral disorganization that prevents goal-directed activity; or catatonic states — waxy flexibility, stupor, mutism, rigid posturing, or stereotyped purposeless movement.
5. Negative symptoms — The absence or reduction of normal functions: flat or blunted affect (minimal emotional expression in face, voice, and manner); alogia (sparse, brief speech with little content); avolition (inability to initiate or persist in goal-directed activity); anhedonia (reduced capacity to experience pleasure); asociality (little desire for social interaction). Negative symptoms are often the most persistent and most disabling features of schizophrenia, and the least responsive to antipsychotic medication.
Criterion B — Significant decline in functioning in work, interpersonal relationships, or self-care, compared to the level before onset.
Criterion C — Continuous signs of the disturbance for at least 6 months, with at least 1 month of active Criterion A symptoms. Prodromal and residual periods (where only negative symptoms or attenuated forms of positive symptoms are present) count toward this 6-month threshold.
Criterion D — Schizoaffective disorder and depressive or bipolar disorder with psychotic features have been excluded.
Criterion E — The disturbance is not attributable to substances (stimulant psychosis, cannabis-induced psychosis) or another medical condition (autoimmune encephalitis, neurological conditions).
Criterion F — If autism spectrum disorder or childhood communication disorder is present, hallucinations or delusions must have been present for at least 1 month in addition to other required criteria.
Signs You Might Have Schizophrenia or Psychosis
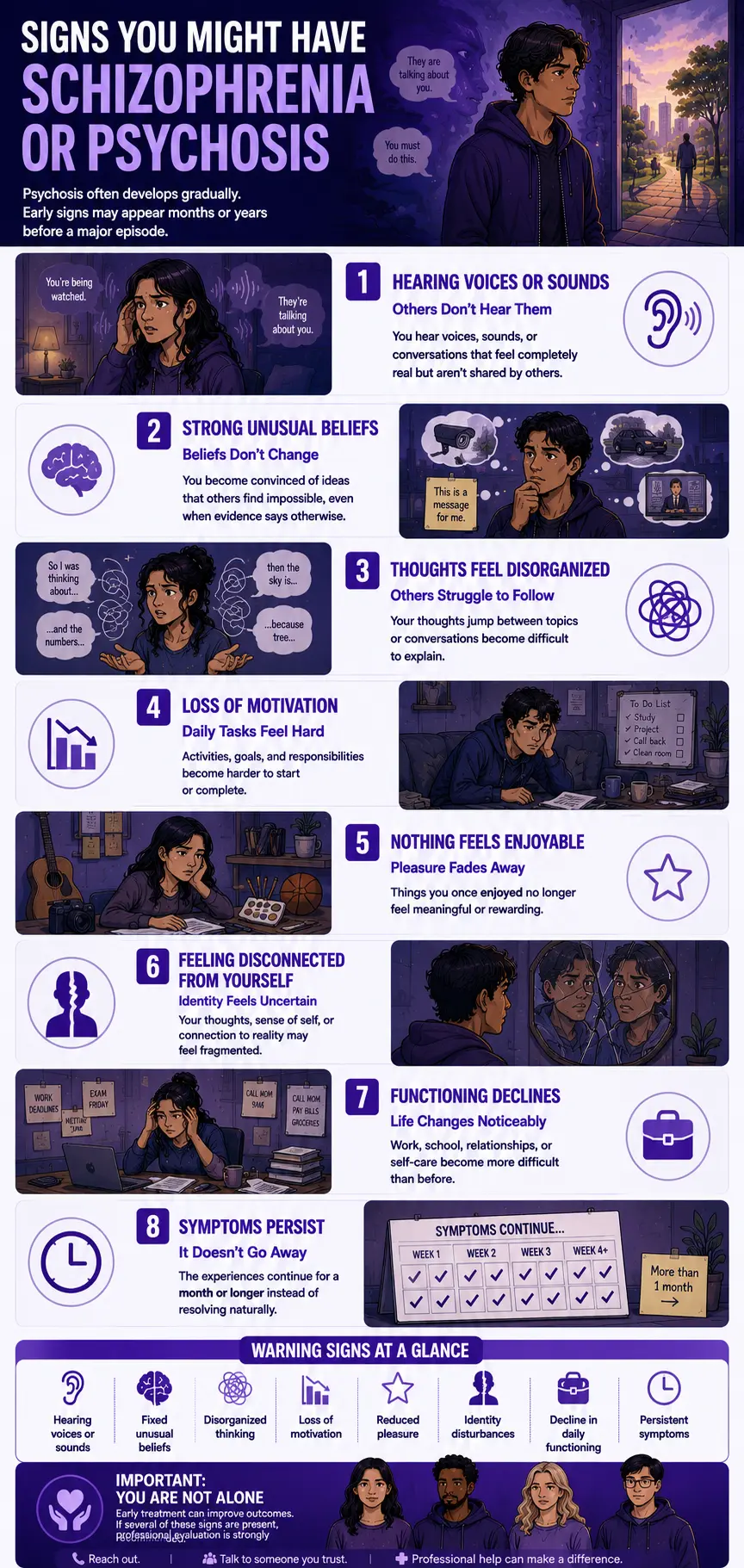
Psychosis and schizophrenia frequently develop gradually — through a prodromal period that may last months or years before a first florid psychotic episode. These are the patterns that most consistently indicate schizophrenia or a psychosis-spectrum condition may be present or developing. If several of these resonate, professional evaluation is important.
You are hearing sounds, voices, or experiences that others don’t seem to share. Auditory hallucinations are the most common symptom of schizophrenia — present in approximately 70% of cases. They may begin as sounds, evolve into words, and become voices that comment on your behavior, converse about you in third person, or issue instructions. The voices feel external and real, not like imagination. If you are hearing voices that others cannot hear, this warrants urgent professional attention regardless of any other symptoms.
You hold beliefs that others find strange, impossible, or untrue — and evidence doesn’t change them. Delusions are fixed false beliefs that persist despite clear contradicting evidence. What makes them distinct from unusual or idiosyncratic beliefs is their fixity and their resistance to challenge — the belief doesn’t update when you encounter evidence against it. Common forms include the belief that you are being followed or monitored, that random events carry specific messages meant for you (ideas of reference), or that you have special powers or a unique mission.
Your thoughts seem to move in ways that don’t quite connect — or others say they can’t follow your thinking. Disorganized thinking — formal thought disorder — manifests as speech that jumps between topics without clear connection, responses that circle around the point without arriving at it, or, in severe cases, sentences that assemble words without coherent meaning. The person is typically unaware of the disorganization; it is more visible to others in conversation than from the inside.
You have noticed a significant loss of motivation, emotional expression, or pleasure over time. Negative symptoms are often the first signs of schizophrenia — appearing in the prodromal period before positive symptoms emerge. A loss of interest in previously valued activities, an increasing flatness of emotional expression, a withdrawal from social connection, or a reduced capacity to feel pleasure may appear gradually and be attributed to depression, laziness, or personality change before the full clinical picture becomes clear.
Things that used to feel meaningful no longer do — including people and activities you previously cared about. Anhedonia — the reduced capacity for pleasure — and asociality — reduced desire for social connection — are core negative symptoms that significantly impair quality of life and are often the most painful features of schizophrenia for the person experiencing them. They are not a choice or a character trait — they are symptoms.
Your sense of yourself — your identity, your continuity, your boundaries — feels fragmented or uncertain. Schizophrenia can produce a profound disruption in the sense of self — the experience that one’s thoughts are being inserted by an outside force, that one’s identity is fragmenting, or that the boundary between self and world is becoming unclear. These experiences — called “first rank” symptoms in the older literature — are distressing and often difficult to describe.
You have been functioning significantly less well than you were before — at work, in relationships, in daily self-care. Criterion B of the DSM-5-TR specifically requires a significant decline in functioning. This is not about comparison to other people but to your own previous level — a decline from where you were before these experiences began. If people who know you have noticed a significant change, that observation is clinically meaningful.
These experiences have been building or recurring over the past month or longer. A single brief, unusual experience may reflect stress, sleep deprivation, or the effects of substances. Schizophrenia requires a minimum of 1 month of active symptoms (Criterion C). The persistence and recurrence of these experiences — their refusal to simply resolve — is an important signal.
Schizophrenia vs Schizoaffective vs Schizotypal vs Brief Psychotic Disorder
| Feature | Schizophrenia | Schizoaffective Disorder | Schizotypal PD | Brief Psychotic Disorder |
|---|---|---|---|---|
| Core symptoms | ≥2 of 5 Criterion A symptoms (delusions, hallucinations, disorganized speech, disorganized behavior, negative symptoms); ≥1 must be the first three | Same psychotic symptoms as schizophrenia PLUS a major mood episode (MDE or manic) that co-occurs for a substantial portion of the illness | Odd beliefs, magical thinking, ideas of reference, unusual perceptions — below the threshold of frank psychosis; personality disorder, not psychotic disorder | Same positive symptoms as schizophrenia but lasting only 1 day to 1 month, with full return to previous functioning |
| Duration | ≥6 months total, with ≥1 month active symptoms | Same duration requirements as schizophrenia; mood episode criteria met for a substantial portion | Chronic — begins by early adulthood and persists; not episodic | 1 day to 1 month; by definition, it resolves within 1 month |
| Mood component | Mood episodes may occur but are brief relative to total illness duration | Mood episode is a substantial and defining feature alongside the psychosis | Not a primary feature; depression is common as a comorbidity | May be triggered by severe stress; no specific mood episode requirement |
| Prognosis | Chronic; variable — some people achieve sustained remission, many have ongoing symptoms; early treatment significantly improves outcomes | Better than schizophrenia, worse than mood disorders alone; the mood component means more treatment targets | Stable personality pattern; few develop full schizophrenia; depression is a primary comorbidity risk | Best prognosis of the spectrum; full recovery expected within 1 month by definition |
| DSM-5-TR code | 295.90 (F20.9) | 295.70 (F25.x) | 301.22 (F21) | 298.8 (F23) |
| PsyMed test | This test | This test + Bipolar Test | Schizotypal PD Test | This test + Anxiety Test |
What Causes Schizophrenia?
The causes of schizophrenia are not fully known, but the weight of evidence points to a multifactorial model combining genetic vulnerability with environmental triggers that affect neurodevelopment (Medscape, 2025; StatPearls, Hany & Rizvi, 2024).
Genetic factors. Schizophrenia is among the most heritable psychiatric conditions — with heritability estimates around 80%. First-degree relatives of people with schizophrenia have a 10-fold increased risk compared to the general population. Genome-wide association studies have identified multiple genetic loci, though no single gene determines the outcome. Shared genetic architecture with bipolar disorder, ADHD, and other psychiatric conditions has been documented. Increased paternal age is associated with greater schizophrenia risk, likely due to de novo mutations (Medscape, 2025).
Dopamine dysregulation. The dopamine hypothesis remains the most influential neurobiological model — specifically, hyperactivity of mesolimbic dopaminergic pathways (producing positive symptoms) alongside hypodopaminergia in the prefrontal cortex (producing negative and cognitive symptoms). All currently effective antipsychotic medications work primarily through dopamine D2 receptor blockade, supporting this model. More recent research implicates glutamate and GABA systems as well.
Neurodevelopmental factors. Evidence consistently supports a neurodevelopmental model — disruptions in fetal brain development (from infections, nutritional deficiencies, obstetric complications, or stress during critical periods) produce vulnerabilities that are expressed clinically in early adulthood when the brain undergoes the final stages of maturation. Urban birth, migration, and minority status are associated with elevated risk — possibly through social stress and urbanicity effects on dopamine sensitivity.
Environmental precipitants. Cannabis use — particularly high-potency THC — is an established environmental risk factor for psychosis and schizophrenia in genetically vulnerable individuals. Stimulant use can precipitate psychosis that may trigger a schizophrenia-spectrum episode. Severe psychosocial stress and trauma exposure are also documented risk factors.
Comorbidities. Approximately 50% of people with schizophrenia have a lifetime history of substance use disorder (DSM-5-TR). Depression and anxiety disorders are among the most common comorbidities (TherapyRoute, 2025). OCD co-occurs in approximately 10–15% of people with schizophrenia. Metabolic syndrome is common as a side effect of antipsychotic treatment and contributes to reduced life expectancy (StatPearls, 2024).
How This Test Works
This Schizophrenia Test screens for the five Criterion A symptom domains — delusions, hallucinations, disorganized speech/thinking, disorganized behavior, and negative symptoms — as well as functional decline, chronicity, and the impact of these experiences on daily life. It is not the PCL-5 or any other formally validated instrument — it is a DSM-5-TR-based screening tool designed to help identify whether a professional evaluation is warranted.
Answer based on your experience over the past month. Answer honestly — this Schizophrenia test is private, and the value lies in accurate self-assessment.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. This is a screening tool. Only a psychiatrist can diagnose schizophrenia, and diagnosis requires a comprehensive evaluation including history, mental status examination, medical workup, and collateral information.
Understanding Your Schizophrenia Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Psychosis Indicators | Responses suggest few significant psychosis or schizophrenia symptoms at this time. Occasional unusual experiences may be present without a pattern consistent with schizophrenia spectrum disorders. |
| 16 – 30 | Mild — Some Psychosis-Related Symptoms Present | Some psychosis-related symptom patterns present across one or more domains. Warrants professional discussion. Early evaluation significantly improves outcomes. |
| 31 – 45 | Moderate — Significant Psychosis Symptom Pattern | Significant psychosis-related symptoms across multiple domains. Consistent with a schizophrenia spectrum presentation. Psychiatric evaluation is strongly recommended as soon as possible. |
| 46 – 60 | High — Strong Psychosis Indicators — Please Seek Help | Severe and pervasive psychosis-related symptoms across most domains. Please seek psychiatric evaluation urgently. If you are in crisis or experiencing command hallucinations, please contact 988 or go to your nearest emergency room. |
Treatment for Schizophrenia
Schizophrenia is a treatable condition. The evidence base for treatment has expanded substantially over the past three decades, and most people with schizophrenia achieve meaningful improvement with appropriate care (MSD Manual, 2026; StatPearls, 2024).
Antipsychotic medications. The cornerstone of schizophrenia treatment. Second-generation (atypical) antipsychotics — including risperidone, olanzapine, quetiapine, aripiprazole, and clozapine — are generally first-line. They reduce positive symptoms in approximately 70–80% of patients. Clozapine is reserved for treatment-resistant schizophrenia (lack of response to two adequate antipsychotic trials) and has the strongest evidence base for this population. Long-acting injectable (LAI) antipsychotics are an important option for people who have difficulty with daily oral medication adherence.
Cognitive Behavioral Therapy for Psychosis (CBTp). An evidence-supported psychological treatment that helps people evaluate and modify the beliefs and coping patterns that maintain distressing psychotic experiences. CBTp does not eliminate hallucinations or delusions but can reduce their distress, improve functioning, and build skills for managing residual symptoms. Recommended alongside antipsychotic treatment by NICE guidelines and increasingly by US practice guidelines.
Coordinated Specialty Care (CSC). A team-based model for early psychosis that combines antipsychotic treatment, CBTp, case management, supported employment and education, family psychoeducation, and peer support. Evidence consistently shows CSC produces better outcomes than standard care for first-episode psychosis. SAMHSA provides a national directory of CSC programs in the United States.
Family psychoeducation. Programs such as NAMI Family-to-Family and structured family psychoeducation interventions significantly reduce relapse rates, improve medication adherence, and improve outcomes for family caregivers. Family involvement in treatment is associated with a better long-term prognosis.
Supported employment and education. Given the significant functional impact of schizophrenia on occupational and educational achievement, supported employment programs (Individual Placement and Support — IPS model) have strong evidence for improving employment outcomes even in people with significant symptoms.
Frequently Asked Questions
What is schizophrenia?
Schizophrenia is a serious, chronic psychiatric disorder (DSM-5-TR 295.90 / F20.9) characterized by positive symptoms (hallucinations, delusions, disorganized thinking and behavior), negative symptoms (flat affect, avolition, alogia, anhedonia, asociality), and cognitive impairments affecting memory, executive function, and processing speed. Diagnosis requires ≥2 of 5 Criterion A symptoms for ≥1 month (at least one being delusions, hallucinations, or disorganized speech), with continuous signs for ≥6 months and significant functional decline. It affects approximately 24 million people globally (1 in 300) and approximately 0.3–0.7% of the population in their lifetime (APA, 2022).
What is the difference between schizophrenia and schizoaffective disorder?
Schizoaffective disorder (DSM-5-TR 295.70 / F25.x) involves the same psychotic symptoms as schizophrenia — delusions, hallucinations, disorganized speech — but with a major mood episode (major depressive episode or manic episode) that is present for a substantial portion of the total illness duration. In schizophrenia, mood episodes may occur but are brief relative to the full illness duration. Schizoaffective disorder generally has a better prognosis than schizophrenia but a more complex treatment picture because both the psychotic and mood components need to be addressed.
Is schizophrenia the same as multiple personality disorder?
No — this is one of the most persistent and damaging misconceptions about schizophrenia. Schizophrenia involves a break from shared reality through hallucinations, delusions, and disorganized thinking — not the presence of multiple distinct personalities. Multiple personality disorder is now called Dissociative Identity Disorder (DID) and is an entirely different condition, categorized under dissociative disorders rather than psychotic disorders. The confusion traces to the etymological origin of “schizophrenia” (Eugen Bleuler, 1911 — “split mind”), which referred to the fragmentation of mental processes, not to multiple selves. The two conditions have different causes, symptom profiles, treatments, and prognoses.
What are the early signs of schizophrenia?
Schizophrenia typically develops through a prodromal period — a phase of gradually building symptoms that precedes the first florid psychotic episode. Early signs include: subtle changes in thinking (ideas that feel significant or connected in unusual ways); social withdrawal and declining function at school or work; a change in the quality of emotional experience; unusual perceptual experiences (fleeting voices, unusual sensory states); odd or eccentric behavior that represents a change from the person’s previous pattern; and deterioration in self-care. These prodromal features may be present for months or years before a first psychotic episode. Early identification during the prodromal phase allows for intervention before full psychosis develops.
Can schizophrenia be treated?
Yes — schizophrenia is treatable, and most people with schizophrenia achieve meaningful improvement with appropriate care. Antipsychotic medications reduce positive symptoms in approximately 70–80% of patients. Cognitive Behavioral Therapy for psychosis (CBTp) reduces distress from residual symptoms and improves functioning. Coordinated Specialty Care programs produce better outcomes than standard care for first-episode psychosis. Early treatment significantly improves long-term prognosis — the MSD Manual (2026) notes that patients treated early “respond more quickly and fully.” Recovery is possible; many people with schizophrenia achieve sustained remission and lead fulfilling lives.
How is schizophrenia different from schizotypal personality disorder?
Schizotypal Personality Disorder (DSM-5-TR 301.22 / F21) exists on the schizophrenia spectrum but is classified as a personality disorder, not a psychotic disorder. STPD involves odd beliefs, magical thinking, ideas of reference, unusual perceptual experiences, eccentric behavior, and severe social anxiety — but these remain below the threshold of frank psychosis. The unusual beliefs in STPD are not fixed delusions; the perceptual experiences are not full hallucinations. STPD is a chronic, stable personality pattern; schizophrenia involves acute psychotic episodes requiring a different level of clinical intervention. The Schizotypal Personality Disorder Test provides a more detailed assessment of that specific presentation.
What resources are available for people with schizophrenia and their families?
The National Alliance on Mental Illness (NAMI) offers extensive resources, including a helpline (1-800-950-NAMI), the Family-to-Family education program, and local support groups: nami.org. SAMHSA provides a national directory of Coordinated Specialty Care programs for early psychosis and a treatment locator: samhsa.gov. The Schizophrenia and Psychosis Action Alliance offers peer support and advocacy resources. For immediate crisis support, call or text 988. In the United Kingdom, Mind and Rethink Mental Illness provide equivalent resources.
Related Tests
- Schizotypal Personality Disorder Test — the most important companion; STPD is on the schizophrenia spectrum but below the threshold of frank psychosis; important to distinguish
- Dissociative Identity Disorder Test — DID is frequently confused with schizophrenia; distinct conditions with different symptoms, mechanisms, and treatments
- Bipolar Test — bipolar disorder with psychotic features can present similarly to schizophrenia; a critical differential that affects the treatment approach
- Paranoid Personality Disorder Test — paranoid ideation below the threshold of delusions; important Cluster A differential
- Borderline Personality Disorder Test — BPD can include transient, stress-related psychotic symptoms; important differential, particularly in younger women
- Clinical Depression Test — depression with psychotic features is a critical differential; depression is also one of the most common schizophrenia comorbidities
- Anxiety Test — anxiety disorders are among the most common schizophrenia comorbidities; approximately 50% of people with schizophrenia have a co-occurring mental health condition
- OCD Test — OCD co-occurs in approximately 10–15% of people with schizophrenia; obsessional thoughts can sometimes be misidentified as psychotic content
- Suicidal Ideation Test — schizophrenia carries a suicide rate of approximately 10%; please assess if any thoughts of self-harm are present
- Anhedonia Test — anhedonia is a core negative symptom of schizophrenia; worth assessing separately alongside this test
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Schizophrenia 295.90 (F20.9), pp. 114–122. psychiatry.org
- Hany, M., & Rizvi, A. (2024). Schizophrenia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. NBK539864. Updated February 23, 2024. [1% global; 13–15 year life expectancy reduction] ncbi.nlm.nih.gov
- MSD Manual Professional Edition. (2026). Schizophrenia. [Early treatment improves response; criteria summary] msdmanuals.com
- World Health Organization. (2022). Schizophrenia Fact Sheet. [24 million globally; 1 in 300] who.int
- TherapyRoute. (2025). Schizophrenia: 2025 Statistics. [0.25–0.64% US; 1 in 222 adults; top 15 causes of disability; 50% co-occurring] therapyroute.com
- Larsen, T.K., Melle, I., Auestad, B., et al. (2011). Early detection of psychosis: positive effects on 5-year outcome. Psychological Medicine, 41(7), 1461–1469. doi.org/10.1017/S0033291710002023
- Rami, A. (2025). Impact of the age of onset and duration of schizophrenia on the quality of treatment adherence. European Psychiatry. [Average onset age 22.91 years; DUP ~2 years] pmc.ncbi.nlm.nih.gov
- Medscape. (2025). Schizophrenia: Background, Diagnostic Criteria (DSM-5-TR), Epidemiology. [Male vs female onset; estrogen hypothesis; paternal age risk] emedicine.medscape.com
- National Alliance on Mental Illness (NAMI). Schizophrenia. nami.org
- Wikipedia. (2025). Schizophrenia. [Lifetime prevalence 0.3–0.7%; 24 million; suicide rate; substance comorbidity] en.wikipedia.org