
The experience most people with schizotypal personality disorder describe is not one of not wanting connection — it is one of connection that never quite forms the way it does for other people. The relationships don’t deepen. The conversations carry undertones others don’t seem to notice. The thoughts run in unusual directions. And the anxiety in social situations doesn’t ease with familiarity the way shyness does — it persists, rooted not in ordinary self-consciousness but in something more specific: a sense that the social world is operating according to rules and meanings that are partly hidden, and that you are reading them differently from everyone else.
Schizotypal Personality Disorder sits at a unique intersection — officially classified as a Cluster A personality disorder in the DSM-5-TR, but reclassified under the schizophrenia spectrum in the ICD-11 — a positioning that reflects its biological and genetic proximity to schizophrenia while acknowledging that most people with STPD do not develop psychosis (StatPearls, Francois & Torrico, 2024). Understanding it requires holding both of those realities simultaneously.
This free Schizotypal Personality Disorder test screens for Schizotypal Personality Disorder using all nine DSM-5-TR diagnostic criteria (APA, 2022). 10 questions. Based on the past 12 months. Instant, private results.
What Is Schizotypal Personality Disorder?
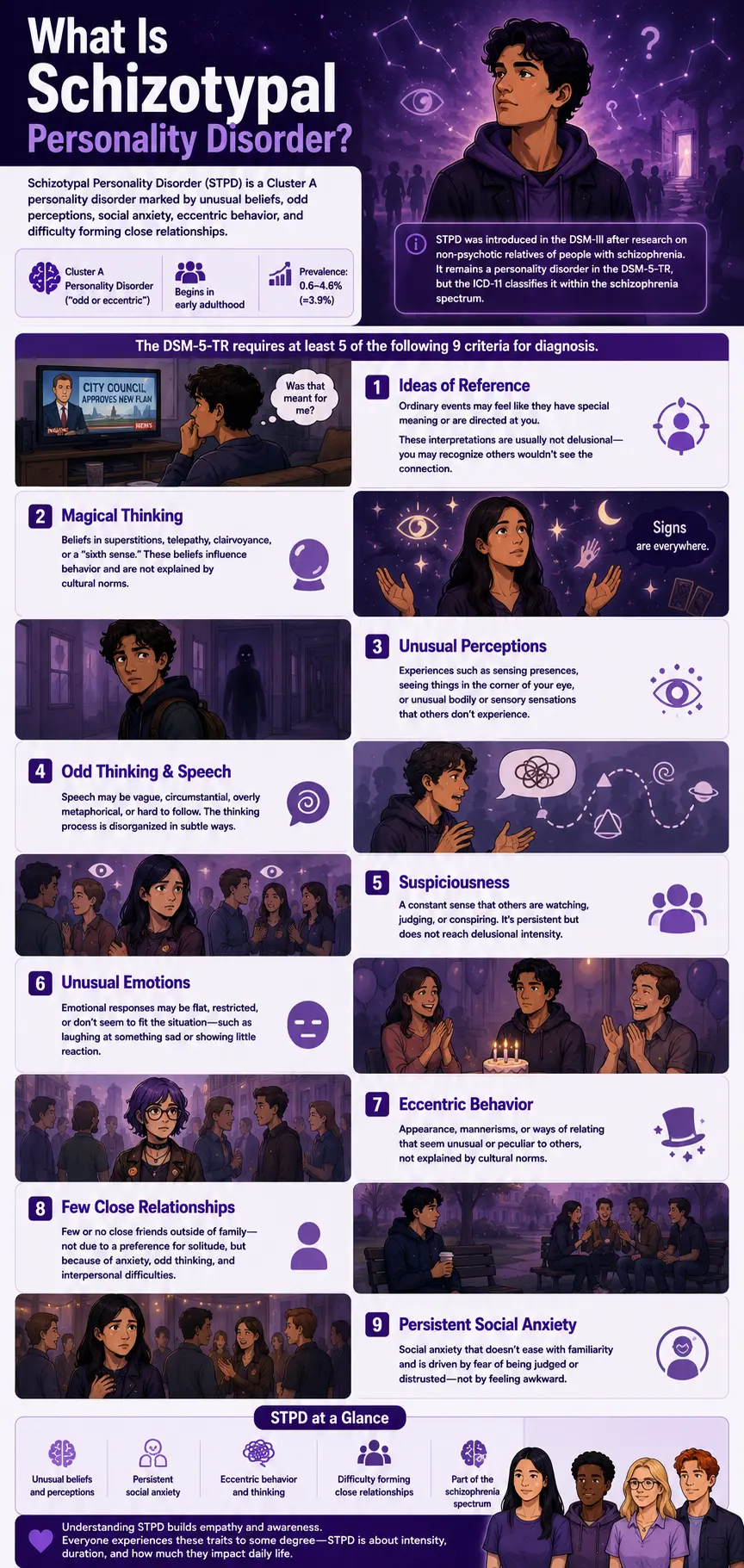
Schizotypal Personality Disorder (STPD) is a Cluster A personality disorder (DSM-5-TR code 301.22 / ICD-10: F21) — grouped alongside Paranoid Personality Disorder and Schizoid Personality Disorder under the “odd or eccentric” cluster. The DSM-5-TR defines it as a pervasive pattern of social and interpersonal deficits characterized by acute discomfort with and reduced capacity for close relationships, cognitive or perceptual distortions, and eccentricities of behavior, beginning in early adulthood and present across a variety of contexts (APA, 2022).
STPD was introduced in the DSM-III, emerging from research studying non-psychotic family members of individuals with schizophrenia — recognizing that a distinct, milder schizophrenia-spectrum presentation existed in the population without meeting the threshold for a psychotic disorder (StatPearls, Francois & Torrico, 2024). The diagnostic designation has been debated since: the DSM-5-TR retains STPD as a personality disorder, while the World Health Organization reclassified it as a form of schizophrenia in the ICD-11, reflecting its biological proximity to the schizophrenia spectrum.
Prevalence estimates range from 0.6–4.6% of the general population (PsychDB, 2024), with a commonly cited figure of approximately 3.9% based on Pulay and colleagues’ (2009) National Epidemiologic Survey on Alcohol and Related Conditions (cited in the Merck Manual, 2026). STPD is more common in males than in females (PsychDB, 2024; StatPearls, 2024).
The DSM-5-TR requires at least 5 of the following 9 criteria for diagnosis (APA, 2022):
Criterion 1 — Ideas of Reference. Incorrect interpretations of causal incidents and external events as having particular and unusual meaning specifically for oneself. Importantly, these are not delusions — the person can usually acknowledge that the interpretation may not be accurate. A random comment overheard in a crowd, a particular sequence of events, a news story — these may feel specifically directed at or connected to oneself in a way that others don’t share.
Criterion 2 — Odd Beliefs or Magical Thinking. Beliefs that are inconsistent with subcultural norms — superstitions, belief in clairvoyance, telepathy, or a “sixth sense,” or, in the case of children, bizarre fantasies or preoccupations. These beliefs influence behavior and are not explained by cultural context.
Criterion 3 — Unusual Perceptual Experiences. Including bodily illusions — sensing presences that aren’t there, seeing things in peripheral vision, experiencing unusual sensory states that fall short of hallucinations but are more than ordinary misperception.
Criterion 4 — Odd Thinking and Speech. Speech that is vague, circumstantial, metaphorical, overelaborate, or stereotyped — in ways that others find hard to follow or describe as unusual. The thinking process, not just the content, is disorganized in subtle ways.
Criterion 5 — Suspiciousness or Paranoid Ideation. A pervasive suspicion toward others — the sense that people are watching, judging, or conspiring — that falls short of delusional intensity but is persistent and influences how the person navigates social contexts.
Criterion 6 — Inappropriate or Constricted Affect. Emotional responses that appear restricted, flat, or that seem mismatched to the situation — laughing at something sad, responding with emotional blankness to something that would typically produce a visible reaction.
Criterion 7 — Odd or Eccentric Behavior or Appearance. Dress, grooming, mannerisms, or ways of relating that strike others as unusual, peculiar, or eccentric — not explained by cultural or subcultural norms.
Criterion 8 — Lack of Close Friends or Confidants. Few or no close friendships outside of first-degree relatives — not due to preference for isolation (as in Schizoid PD) but due to the anxiety, distorted cognition, and interpersonal difficulties that prevent close relationships from forming or sustaining.
Criterion 9 — Excessive Social Anxiety. Social anxiety that does not diminish with familiarity — unlike ordinary shyness, which eases as situations become known — and that tends to be associated with paranoid fears rather than negative self-judgment. The anxiety persists not because “I am awkward” but because “I am not sure these people can be trusted.”
Signs You Might Have Schizotypal Personality Disorder
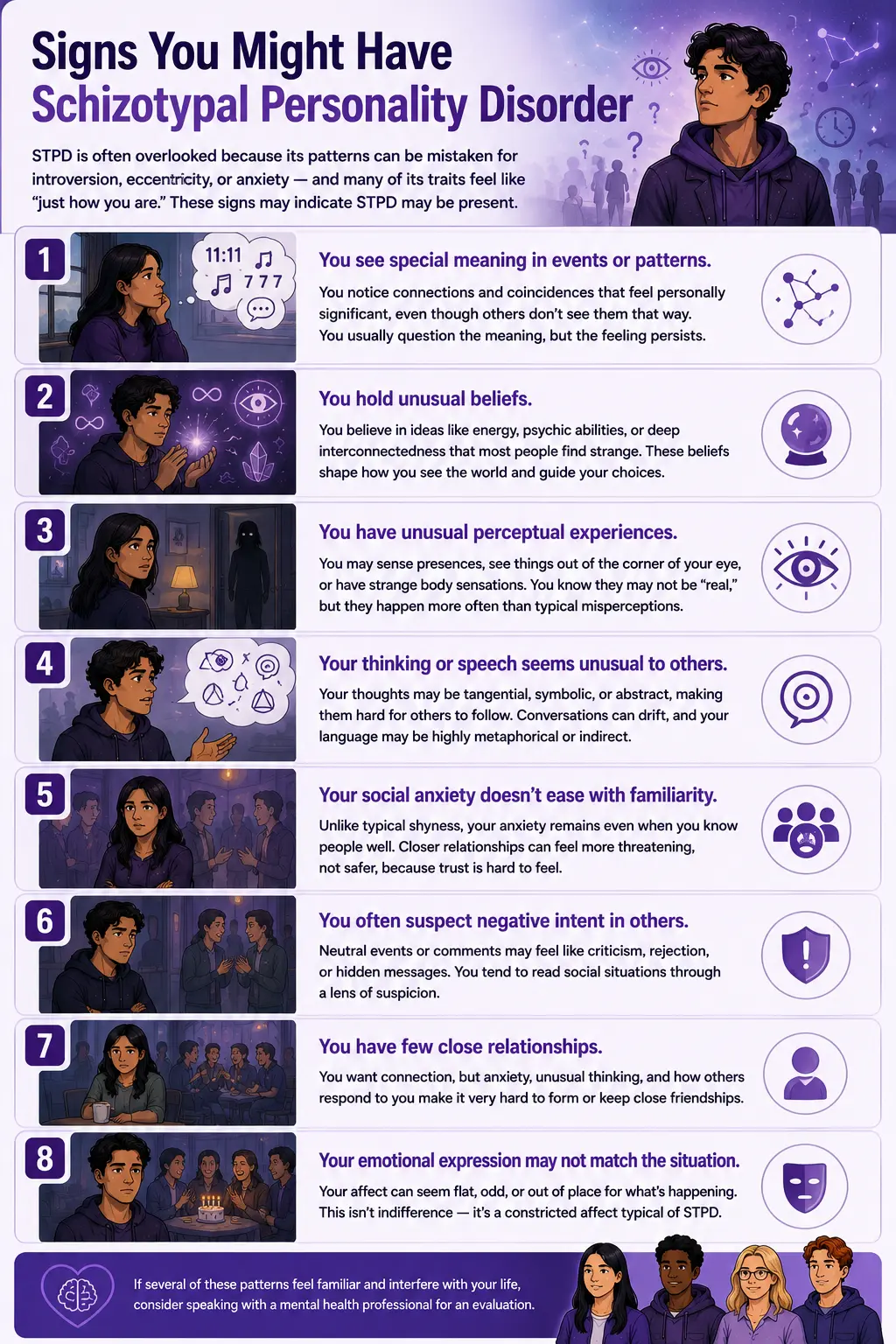
STPD is frequently unrecognized — both because its presentation is easily attributed to introversion, eccentricity, or anxiety, and because many of its features are ego-syntonic (experienced as simply how one thinks rather than as symptoms). These are the patterns that most consistently indicate STPD may be present:
You regularly notice connections between events, coincidences, or patterns that seem to carry specific meaning — but that others don’t share or find significant. This is ideas of reference — not a delusion (you may well question whether the interpretation is accurate), but a persistent perceptual tendency to see personal significance in neutral or random events. A particular song on the radio when you’re thinking of someone, a sequence of numbers that keeps appearing, an overheard conversation that seems to directly address something you’ve been worried about. The connections feel real and meaningful in a way that is difficult to fully dismiss.
You hold beliefs — about consciousness, energy, invisible forces, or the interconnectedness of things — that most people around you don’t share and may find strange. These may be religious or spiritual beliefs that go significantly beyond mainstream faith, beliefs in psychic abilities, precognition, or the capacity of the mind to influence physical reality. They influence your decisions and your interpretation of events. They are not a casual curiosity but a genuine framework through which you navigate the world.
You sometimes experience unusual perceptual states — sensing a presence in a room, seeing something in peripheral vision, feeling as though your body is behaving in an unusual way. These fall short of hallucinations — they are ambiguous, often brief, and you are usually aware they may not be “real” in the conventional sense. But they are more than ordinary misperceptions and occur with some regularity.
People sometimes describe your speech or thinking as unusual — tangential, overly symbolic, hard to follow, or strangely abstract. You may struggle to communicate your thoughts in a linear way, not because the thoughts are unclear to you but because they don’t organize themselves along the paths that most people’s thinking follows. Conversations may drift into territory others don’t follow. Your language may be unusually metaphorical or elliptical.
Social anxiety that does not ease when you know people better. Ordinary social anxiety tends to reduce with familiarity — once you know someone, the anxiety about them diminishes. In STPD, the anxiety often does not ease in this way. If anything, closer relationships can feel more threatening rather than safer — because the concerns are not primarily about performance or embarrassment but about trust, intention, and whether the relationship is what it appears to be.
You tend to interpret neutral events or comments as having negative intent toward you. The absence of a response to a message that could simply mean the person is busy may feel like a deliberate snub. A seemingly neutral comment may register as coded criticism. This perceptual tendency — toward suspicious interpretation of ambiguous social information — is distinct from the hostile attribution bias of IED or the persecution of clinical paranoia, but it shapes social interactions in significant and often isolating ways.
You have very few close relationships and have had few throughout your life. Unlike schizoid personality disorder, where the isolation is preferred and ego-syntonic, in STPD the lack of close relationships is typically experienced as a loss — you want the connection, but the combination of anxiety, distorted cognition, and others’ responses to your eccentricities makes it consistently difficult to form or maintain.
Your affect — your visible emotional expression — sometimes mismatches the situation in ways you may not fully notice. Others may describe you as flat, cold, or emotionally strange in situations that would typically produce visible warmth or distress. This is not indifference; it is the constricted affect that characterizes STPD, distinct from the genuine indifference of schizoid personality disorder.
STPD vs Schizoid vs Paranoid — The Critical Distinctions
The three Cluster A disorders are frequently confused. Understanding what distinguishes them is clinically important because the underlying dynamics differ significantly despite surface similarities.
| Feature | Schizotypal PD (STPD) | Schizoid PD | Paranoid PD (PPD) |
|---|---|---|---|
| Desire for relationships | Present — wants connection but cannot sustain it due to anxiety and distorted cognition | Absent — genuinely indifferent to relationships; prefers isolation | Variable — relationships are approached with sustained suspicion and distrust |
| Cognitive distortions | Prominent — ideas of reference, magical thinking, unusual beliefs, perceptual distortions | Absent — thinking is not distorted, just emotionally blunted and socially disengaged | Paranoid ideation predominates but without the odd thinking, magical beliefs, or perceptual distortions |
| Nature of social anxiety | Rooted in paranoid fears and cognitive distortions; does NOT ease with familiarity | Not anxious about social situations — simply disinterested | Fear-based but rooted in specific mistrust of others’ motives, not in generalized perceptual distortion |
| Eccentricity | Prominent — odd speech, appearance, behavior, and thinking | Not typically eccentric — flat and disengaged but not odd | Not eccentric — logical and organized but chronically suspicious |
| Schizophrenia spectrum | Yes — genetically related; ICD-11 classifies as schizophrenia spectrum | Debated — less clearly on the spectrum | Can precede paranoid schizophrenia but less clearly spectrum-related |
| DSM-5-TR code | 301.22 (F21) | 301.20 (F60.1) | 301.0 (F60.0) |
| PsyMed test | This test | Schizoid PD Test | Paranoid PD Test |
A critical clinical note from the Merck Manual (2026): schizotypal personality disorder can be distinguished from paranoid and schizoid personality disorders because patients with those disorders do not have the odd, disorganized thoughts and behavior that characterize STPD. The cognitive and perceptual distortions — ideas of reference, magical thinking, unusual perceptual experiences — are the features most specific to STPD and most important for differential diagnosis.
What Causes Schizotypal Personality Disorder?
The etiology of STPD is thought to be primarily biological, given its position on the schizophrenia spectrum and the evidence for shared genetic architecture with schizophrenia (Merck Manual, 2026).
Genetic factors. STPD was originally conceptualized from research on non-psychotic relatives of schizophrenia patients — recognizing that subclinical schizophrenia-spectrum features ran in families (StatPearls, Francois & Torrico, 2024). Specific genetic candidates include the DTNBP1 gene (which produces dysbindin, a brain protein linked to schizophrenia and paranoid behavior) and the COMT gene (which influences dopamine metabolism and is associated with schizophrenia-spectrum presentations), both of which are shared between STPD and schizophrenia (MD Searchlight, 2024).
Dopaminergic dysregulation. Given the genetic overlap with schizophrenia and the response of some STPD symptoms to low-dose antipsychotics, dopaminergic dysregulation — particularly in the mesolimbic pathway — is implicated in the cognitive and perceptual distortions characteristic of STPD (Merck Manual, 2026; StatPearls, 2024).
Neurodevelopmental factors. STPD shares with schizophrenia a pattern of neurodevelopmental disruption — minor neurological abnormalities, subtle cognitive deficits, and early-onset eccentric behavior that can be detected in childhood before the full personality pattern emerges in early adulthood (DSM-5-TR, APA, 2022).
Environmental factors. Childhood trauma, adverse developmental experiences, and early social isolation may interact with genetic vulnerability to shape the severity of STPD expression. However, environmental factors appear to be secondary to biological ones in STPD etiology — distinguishing it from some other personality disorders where developmental experience plays a more primary role (Merck Manual, 2026).
Comorbidities. STPD has high comorbidity rates. More than half of people with STPD have had at least one episode of major depressive disorder, and 30–50% have MDD at the time of STPD diagnosis (Merck Manual, 2026, citing Pulay et al., 2009). Substance use disorders are also common. Other frequently co-occurring conditions include anxiety disorders, other Cluster A personality disorders, and Borderline Personality Disorder.
How This Test Works
This test screens for Schizotypal Personality Disorder using all nine DSM-5-TR diagnostic criteria (APA, 2022) across 10 questions — covering ideas of reference, magical thinking, unusual perceptual experiences, odd thinking and speech, suspiciousness, constricted or inappropriate affect, odd behavior or appearance, lack of close friends, and the persistent social anxiety that does not ease with familiarity.
Answer based on your consistent experience over the past 12 months — the chronic, recurring pattern rather than specific episodes or your best or worst periods.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–40. This is a screening tool — only a qualified mental health professional can diagnose STPD through a comprehensive clinical assessment that rules out schizophrenia, ASD, and other presentations.
Understanding Your STPD Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 10 | Low — Few STPD Indicators | Responses suggest few significant STPD patterns. Occasional unusual thinking or social discomfort may be present without a pattern consistent with Schizotypal Personality Disorder. |
| 11 – 20 | Mild — Some Schizotypal Patterns Present | Some schizotypal features present across multiple domains. May not reach full STPD threshold, but patterns are meaningful and warrant reflection or professional discussion. |
| 21 – 30 | Moderate — Significant STPD Pattern | Significant schizotypal pattern across multiple DSM-5-TR criteria. Consistent with STPD, professional evaluation is recommended. |
| 31 – 40 | High — Strong STPD Indicators | Pervasive and severe schizotypal pattern across most criteria. Professional evaluation is strongly recommended, including to rule out schizophrenia spectrum conditions. |
Treatment for Schizotypal Personality Disorder
According to the Merck Manual (2026) and StatPearls (Francois & Torrico, 2024), effective approaches include:
Cognitive Behavioral Therapy (CBT). The most evidence-supported psychological treatment. CBT for STPD targets the specific cognitive distortions — ideas of reference, magical thinking, paranoid interpretations of social events — through reality testing, cognitive restructuring, and the gradual development of more accurate social perception. The therapeutic relationship itself is a critical vehicle: many people with STPD have had few close relationships, and the experience of a consistent, trust-based professional relationship can itself be corrective.
Social skills training. Specifically recommended for STPD given the prominence of interpersonal deficits. Group-based social skills training provides both the skills and the graduated social exposure that are most relevant to STPD — building the capacity for close relationships in a structured, low-stakes environment (Merck Manual, 2026).
Low-dose antipsychotics. Particularly risperidone, which has demonstrated efficacy for the cognitive and perceptual symptoms of STPD in controlled studies. Low-dose antipsychotics do not eliminate the schizotypal features but reduce the intensity of the perceptual distortions, the ideas of reference, and the paranoid ideation enough to make psychotherapy more accessible (Merck Manual, 2026).
Antidepressants. For the very high rates of comorbid major depression in STPD (30–50% at the time of diagnosis; Pulay et al., 2009), SSRIs are used adjunctively. Addressing the depression as a separate treatment target improves overall functioning and reduces the negative spiral between depressive withdrawal and STPD isolation.
Frequently Asked Questions
What is Schizotypal Personality Disorder?
Schizotypal Personality Disorder (STPD) is a Cluster A personality disorder (DSM-5-TR 301.22 / F21) defined as a pervasive pattern of social and interpersonal deficits, cognitive or perceptual distortions, and eccentricities of behavior, beginning by early adulthood and present across contexts. Diagnosis requires at least 5 of 9 DSM-5-TR criteria, including ideas of reference, magical thinking, unusual perceptual experiences, odd speech and thinking, suspiciousness, inappropriate or constricted affect, odd behavior or appearance, lack of close friends, and persistent social anxiety associated with paranoid fears. Prevalence ranges from 0.6–4.6% (PsychDB, 2024), with a frequently cited figure of ~3.9% (Pulay et al., 2009). It is more common in males (StatPearls, 2024) and was introduced in the DSM-III from research on non-psychotic relatives of schizophrenia patients.
Is STPD the same as schizophrenia?
No — but the relationship is clinically important. STPD is on the schizophrenia spectrum: it shares genetic architecture with schizophrenia (including DTNBP1 and COMT gene variants), shares some surface features (ideas of reference, unusual perceptual experiences), and was originally identified through research on schizophrenia family members. The critical differences: STPD does not involve frank psychosis — the perceptual distortions and unusual beliefs fall short of hallucinations and delusions. The DSM-5-TR notes that relatively few individuals with STPD develop schizophrenia or another psychotic disorder (StatPearls, Francois & Torrico, 2024). The ICD-11 classifies STPD under the schizophrenia spectrum; the DSM-5-TR retains it as a personality disorder. Both positions reflect real aspects of its nature.
What is the difference between STPD and Schizoid Personality Disorder?
This is one of the most important distinctions in Cluster A. Schizoid PD involves a genuine absence of desire for close relationships — a preference for isolation that is ego-syntonic. STPD involves a desire for connection that is blocked by anxiety, distorted cognition, and others’ responses to eccentricity. Additionally, STPD includes cognitive and perceptual distortions (ideas of reference, magical thinking, unusual beliefs) that Schizoid PD does not — the odd thinking and perception are unique to STPD among the Cluster A disorders. The social anxiety in STPD is also qualitatively different: in Schizoid PD, social situations produce indifference; in STPD, they produce anxiety rooted in paranoid fears that does not ease with familiarity.
Can STPD be confused with Autism Spectrum Disorder?
Yes — and this differential is clinically important. Both STPD and ASD can involve social difficulties, unusual thinking, and eccentric behavior. Key distinguishing features: ASD involves impairment in social communication and reciprocity that is developmental in origin and typically present from early childhood; the social difficulties in ASD stem from a different processing style rather than from anxiety and paranoid distortion. ASD does not typically involve the ideas of reference, magical thinking, or paranoid ideation of STPD. A comprehensive clinical evaluation — including developmental history — is necessary to distinguish the two. The two can also co-occur.
What is the long-term course of STPD?
STPD has a relatively stable course — the pattern tends to persist rather than intensify toward psychosis. The DSM-5-TR notes that relatively few individuals with STPD develop schizophrenia or another psychotic disorder, and StatPearls (Francois & Torrico, 2024) confirms this — while older research suggested frequent progression to schizophrenia, more recent data do not support this. The primary long-term risks are chronic social isolation, depression (comorbid MDD in 30–50% of cases; Merck Manual, 2026), and occupational difficulty rather than psychotic decompensation.
Is STPD treatable?
Yes — STPD is treatable, and meaningful improvement in functioning and quality of life is achievable with appropriate, sustained intervention. CBT targeting cognitive distortions, social skills training, and low-dose antipsychotics for cognitive-perceptual symptoms are the most evidence-supported approaches (Merck Manual, 2026). Treatment is typically long-term given the personality-level nature of the disorder. The primary challenges are engagement — the same paranoid distrust and social anxiety that define STPD make it difficult to establish and maintain a therapeutic relationship — and the ego-syntonic quality of some features, particularly the unusual beliefs and perceptual experiences, which may not be experienced as symptoms by the person holding them.
How does STPD affect relationships?
STPD affects relationships primarily through two mechanisms. First, the anxiety and distorted cognition prevent close relationships from forming or deepening — the paranoid fears, the ideas of reference, and the odd thinking create social distance and responses from others (bewilderment, withdrawal) that reinforce isolation. Second, those relationships that do form are affected by the constricted affect and odd speech — the emotional unavailability and communicative strangeness that make sustained intimacy difficult. Most people with STPD experience the resulting isolation as painful rather than preferred — which is the feature that most clearly distinguishes STPD from Schizoid PD and that most powerfully motivates engagement with treatment when the person understands that their pattern has a name and responds to intervention.
Related Tests
- Schizoid Personality Disorder Test — the most important companion test; both are Cluster A, but Schizoid involves genuine indifference to relationships vs STPD’s anxious, distorted desire for connection
- Paranoid Personality Disorder Test — shares suspiciousness and social distrust with STPD but without STPD’s cognitive distortions, odd thinking, or unusual beliefs
- Cluster B Personality Disorder Test — important to rule out BPD, which can co-occur with STPD and shares some surface features
- Social Anxiety Test — the social anxiety in STPD is qualitatively different from SAD (rooted in paranoid fears vs performance anxiety), but both need to be assessed
- Clinical Depression Test — over 50% of people with STPD have experienced major depression; comorbid MDD in 30–50% at time of diagnosis (Pulay et al. 2009)
- Borderline Personality Disorder Test — BPD can co-occur with STPD; both involve interpersonal instability and identity disturbance, through different mechanisms
- Dissociative Identity Disorder Test — unusual perceptual experiences in STPD should be distinguished from dissociative phenomena
- Anxiety Test — anxiety disorders are common STPD comorbidities and need separate assessment and treatment
- Dark Triad Test — the suspiciousness and social withdrawal of STPD should be distinguished from the strategic coldness of Machiavellianism and subclinical psychopathy
- Full Personality Disorder Test Hub — all ten DSM-5-TR personality disorder types across Clusters A, B, and C
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Schizotypal Personality Disorder 301.22 (F21), pp. 754–759. psychiatry.org
- Francois, Z., & Torrico, T.J. (2024). Schizotypal Personality Disorder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. NBK603720. Updated May 7, 2024. ncbi.nlm.nih.gov
- Merck Manual Professional Edition. (2026). Schizotypal Personality Disorder (STPD). merckmanuals.com
- Pulay, A.J., Stinson, F.S., Dawson, D.A., et al. (2009). Prevalence, correlates, disability, and comorbidity of DSM-IV schizotypal personality disorder. Primary Care Companion to the Journal of Clinical Psychiatry, 11(2), 53–67. [~3.9% prevalence; MDD comorbidity 30–50%] doi.org/10.4088/pcc.08m00679
- PsychDB. (2024). Schizotypal Personality Disorder. [Prevalence 0.6–4.6%; more common in males] psychdb.com
- MD Searchlight. (2024). Schizotypal Personality Disorder. [DTNBP1 and COMT gene variants] mdsearchlight.com
- World Health Organization. (2022). International Classification of Diseases, 11th Revision (ICD-11). Schizotypal disorder — reclassified under the schizophrenia spectrum. icd.who.int
- Wikipedia. (2025). Schizotypal personality disorder. en.wikipedia.org