
Empathy is not a single thing. The word covers at least three psychologically distinct capacities that can exist at very different levels in the same person: the ability to understand what someone else is thinking and feeling — to model their mental state accurately even when it differs from your own; the ability to feel what they are feeling — to resonate with their emotional experience rather than simply knowing about it; and the motivation to respond to both in ways that help rather than ignore. Understanding without feeling produces a cold accuracy. Feeling without understanding produces a flooded, undirected emotionality. Both without prosocial motivation produce knowledge and experience that go nowhere.
The relationship between these three dimensions is what makes empathy genuinely complex to measure — and what makes the question “how empathetic am I?” more nuanced than a simple score can fully capture. This test covers all three dimensions across 15 questions, inspired by the most extensively validated empathy instrument in psychological research.
This free Empathy Test is inspired by the Empathy Quotient (EQ), developed by Dr. Simon Baron-Cohen and Dr. Sally Wheelwright at the Autism Research Centre, University of Cambridge (2004). 15 questions. Instant, private results.
What Is Empathy?
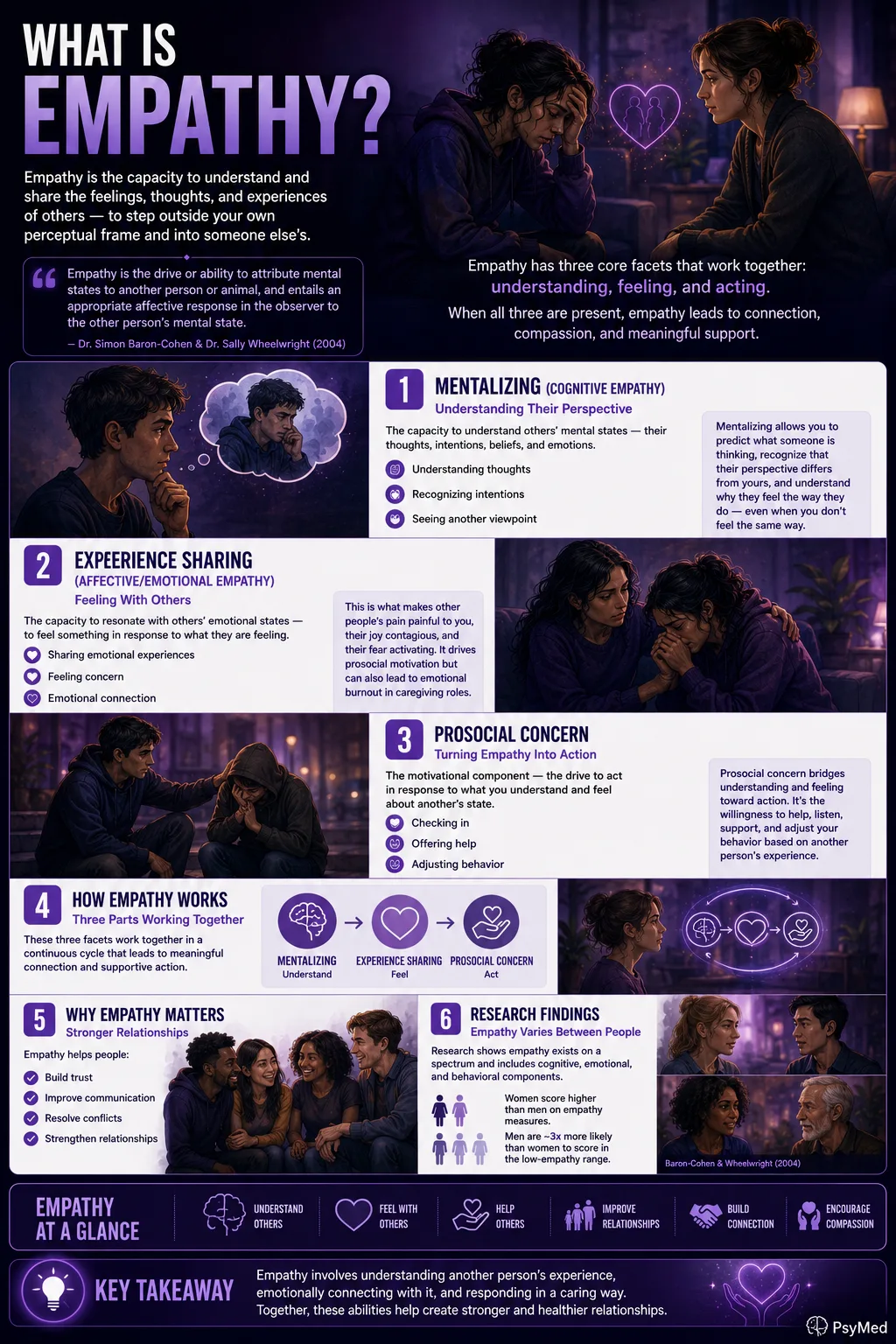
Empathy is the capacity to understand and share the feelings, thoughts, and experiences of others — to step outside your own perceptual frame and into someone else’s. The most scientifically influential definition was provided by Dr. Simon Baron-Cohen and Dr. Sally Wheelwright (2004): “Empathy is the drive or ability to attribute mental states to another person or animal, and entails an appropriate affective response in the observer to the other person’s mental state.” This definition captures both the cognitive dimension (attributing mental states — understanding what another is thinking) and the affective dimension (responding with an appropriate emotion to those mental states — feeling something in response).
The framework developed by Zaki and Ochsner (2012, Nature Neuroscience) identifies three major facets of empathy that have become influential in subsequent research:
1. Mentalizing (Cognitive Empathy)
The capacity to understand others’ mental states — their thoughts, intentions, beliefs, and emotions — accurately and without necessarily sharing them. Mentalizing is what allows you to predict what someone is thinking, recognize that their perspective differs from yours, and understand why they feel the way they do even when you don’t feel the same way yourself. It is closely related to Theory of Mind — the capacity to attribute independent mental states to others. Mentalizing can be intact even when affective empathy is significantly reduced — the narcissist who understands that you are in pain but does not feel moved by it is an example of mentalizing without affective empathy.
2. Experience Sharing (Affective/Emotional Empathy)
The capacity to resonate with others’ emotional states — to feel something in response to what they are feeling, not just to know about it. Affective empathy is what makes other people’s pain painful to you, their joy contagious, their fear activating. It is the component most strongly associated with prosocial motivation — feeling something in response to another’s distress creates the motivation to help. It is also the component most associated with emotional burnout in caregiving roles: experiencing others’ suffering through affective resonance has a cumulative cost.
3. Prosocial Concern
The motivational component — the drive to act in response to what you understand and feel about another’s state. Prosocial concern bridges cognitive and affective empathy toward action: the willingness to check in, to help, to listen, to adjust your behavior based on your understanding of another’s experience. Baron-Cohen’s definition explicitly includes this as a drive component: empathy is not simply having the capacity but also being motivated to use it.
Lawrence and colleagues (2004, Psychological Medicine) validated a three-factor structure of the EQ corresponding to these three facets: Cognitive Empathy, Emotional Reactivity, and Social Skills — mapping directly onto the Zaki-Ochsner framework of mentalizing, experience sharing, and prosocial concern.
Baron-Cohen and Wheelwright (2004) also documented consistent gender differences in empathy: women score significantly higher than men on EQ measures, with non-autistic females averaging approximately 47/80 on the full EQ and males averaging approximately 42/80. Men are also approximately three times more likely than women to score in the low-empathy range.
Signs You May Have Low Empathy
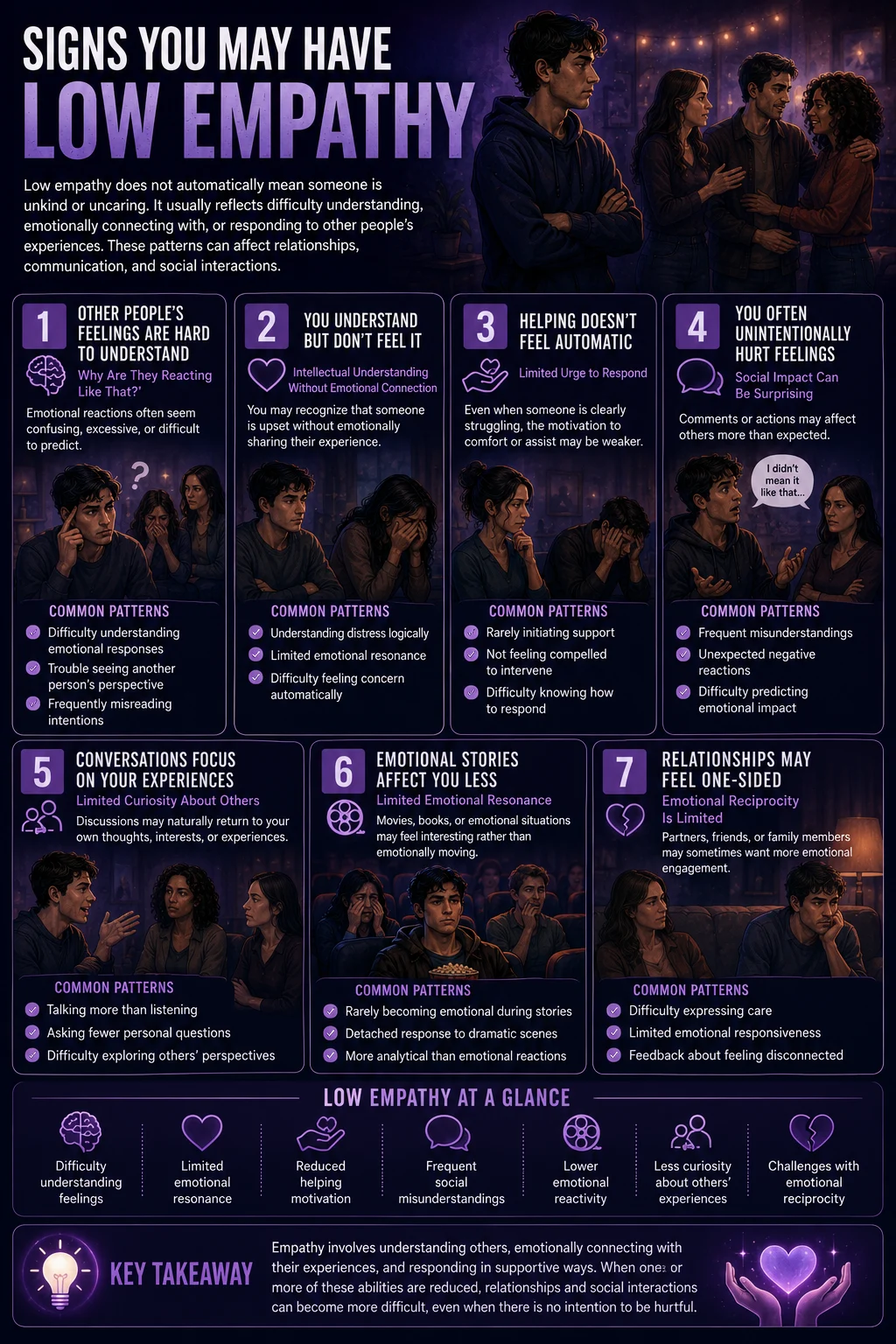
Low empathy is not the same as being unkind. It is possible to behave well toward others without experiencing strong affective resonance with their emotional states. But the absence of empathy — particularly the combination of low cognitive and low affective empathy — exhibits recognizable patterns that consistently affect relationships and social functioning.
You find it difficult to understand why people feel the way they do — their emotional reactions seem disproportionate, irrational, or simply hard to read. This is the cognitive empathy deficit: the reduced capacity to accurately model others’ mental states. When others cry at something that doesn’t move you, feel hurt by something that seems trivial, or become anxious in situations that feel fine to you — the difficulty in attributing those states accurately to their perspective is the cognitive empathy gap. It produces genuine confusion about others’ behavior, which is different from the contempt that may accompany high cognitive empathy with low affective empathy.
Other people’s emotional states don’t register in your own emotional experience — you understand intellectually that someone is upset but don’t feel anything in response. This is the affective empathy deficit — the absence of emotional resonance. You can observe distress accurately without it producing any internal echo. The empathy gap here is not in understanding but in feeling: the other person’s emotional state doesn’t produce an appropriate affective response in you. Research on narcissism has documented this specific profile: “I understand your pain, but I do not feel it” — intact cognitive empathy with significantly reduced affective empathy (Shahri et al., Frontiers in Psychology, 2024).
You don’t typically feel compelled to help, comfort, or respond when someone around you is distressed. This is the prosocial motivation deficit — the reduced drive that converts empathic understanding and feeling into action. Without the motivational component, even accurate mentalizing and some affective resonance don’t translate into helping behavior. The person in front of you is visibly upset; you register it; something in you doesn’t move toward responding.
You are frequently surprised to learn that you have hurt or offended someone. Because cognitive empathy involves the ability to predict how your behavior will land for another person, a cognitive empathy deficit produces a specific kind of interpersonal blind spot: actions that are natural or reasonable from your own perspective may land very differently for the other person, and without the capacity to accurately model their perspective, you don’t anticipate this. The surprise is genuine — which distinguishes low empathy from deliberate unkindness.
In conversations, you primarily discuss your own experiences rather than showing curiosity about others’ experiences. Social curiosity about other people’s inner lives — what they think, how they feel, what they want — is a behavioral expression of empathic motivation. Low prosocial concern produces conversations that are self-referential not through selfishness but through a genuine absence of the pull toward others’ inner lives that drives social curiosity in high-empathy individuals.
You find emotional movies, books, or situations less affecting than others around you describe them being. Low emotional reactivity — the affective empathy dimension — shows up clearly in response to fiction, which is a safe domain for emotional resonance. If movies that move others to tears produce only intellectual appreciation in you, that pattern is consistent with low affective empathy. Baron-Cohen and Wheelwright (2004) used non-emotional engagement with movies as one of the EQ items specifically because it is a common observable expression of affective empathy differences.
Close relationships have been described by others as feeling one-sided or lacking emotional reciprocity. The accumulated effect of reduced empathy in relationships is a specific asymmetry that others experience as the relationship “not going both ways” — their distress doesn’t produce visible caring responses; their joy isn’t shared; their needs don’t seem to register as things that matter. This feedback — whether from partners, friends, or family — is one of the most reliable external indicators of a clinically meaningful empathy deficit.
Signs You May Have High Empathy
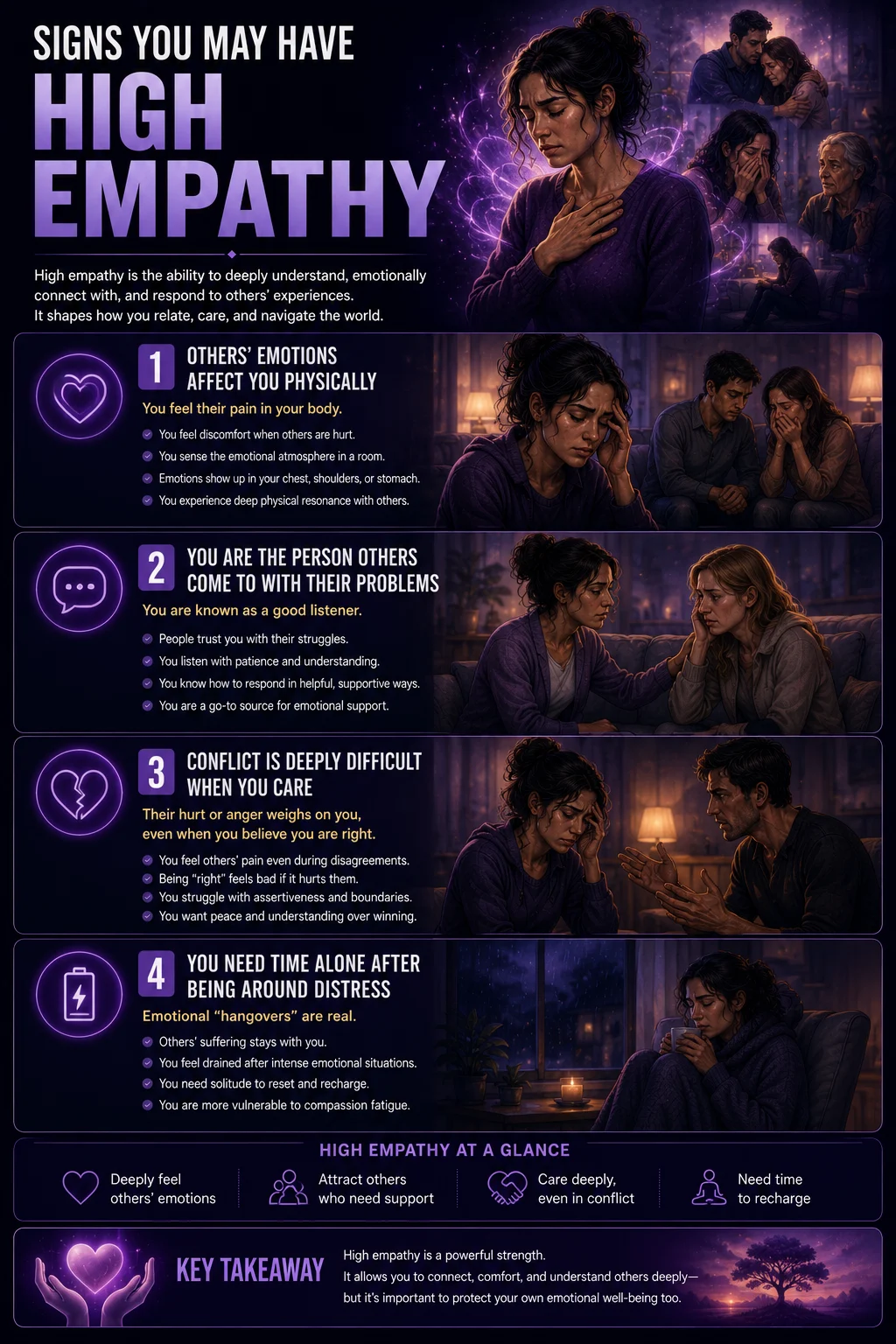
Others’ emotional states affect you physically — you feel their pain in your body. High affective empathy produces somatic resonance: the discomfort of watching someone embarrass themselves, the physical sensation when someone you care about is hurt, the way a room’s emotional atmosphere registers in your chest, shoulders, or stomach. This embodied quality of emotional resonance is the signature of high affective empathy.
You are often the person others come to with their problems — and you are known as a good listener. The social skills dimension of empathy — attending to others, recognizing when they need support, responding in ways they find helpful — produces the relational pattern where you become the go-to person for emotional support across your relationships.
You find it difficult to be in conflict with someone you care about — the sense of their hurt or anger is distressing even when you believe you are right. High affective empathy means that others’ emotional states don’t stop affecting you simply because you disagree with their position or think they are wrong. This produces the characteristic high-empathy conflict pattern: being right feels bad if it means the other person feels bad, which complicates assertiveness and boundary-setting.
You sometimes struggle with the emotional “hangover” after being around people in distress — you need time alone to discharge the emotional resonance. This is the cost of high affective empathy: the resonance doesn’t stop when the situation ends. High-empathy individuals working in caregiving, therapy, medicine, or social work are particularly vulnerable to compassion fatigue — the cumulative depletion that comes from sustained, high-intensity affective resonance with others’ suffering.
Empathy, Low Empathy, and Personality — The Clinical Connections
| Condition | Cognitive Empathy | Affective Empathy | Prosocial Motivation | Overall Profile |
|---|---|---|---|---|
| High Empathy (healthy range) | Strong — accurately reads others’ mental states | Strong — resonates with others’ emotions | Strong — motivated to help and respond | Integrated empathy across all three dimensions |
| Narcissistic Personality Disorder (NPD) | Often intact or even elevated — can read others accurately for strategic purposes | Significantly reduced — “I understand your pain but do not feel it” (Shahri et al. 2024) | Absent when self-interest conflicts — selectively activated for impression management | Cold accuracy without resonance; empathy used as a tool rather than a connection |
| Borderline Personality Disorder (BPD) | Variable — reduced under stress; heightened in some interpersonal contexts | High — often hyper-resonant with others’ emotions; contributes to emotional flooding | Present but impaired by emotional dysregulation — overwhelmed rather than absent | Flooded rather than deficient; empathy is overwhelming rather than absent |
| Psychopathy / ASPD | Can be intact — psychopaths can read others accurately for manipulation | Severely reduced or absent — no resonance with others’ distress | Absent — no prosocial motivation; others’ welfare is irrelevant to decision-making | Most severe empathy deficit; cold accuracy used for exploitation not connection |
| Autism Spectrum (not a disorder of empathy) | Reduced in some contexts — difficulty reading neurotypical social cues | Often intact or high — autistic individuals frequently describe high affective empathy | Present — motivation to help and connect is typically genuine | Double empathy problem — difficulty reading NT cues, not absence of caring |
| Compassion Fatigue / Burnout | Usually intact | Initially high; depleted by chronic resonance — numbing as a protective response | Initially high; depleted — motivation to help exhausted | Empathy exhaustion, not deficit, was present and has been depleted |
An important clinical note on autism and empathy: the autism-empathy relationship is more complex than “autistic people lack empathy.” Research has increasingly documented the double empathy problem (Milton, 2012) — a bidirectional mismatch in which autistic and neurotypical individuals have difficulty understanding each other’s mental states, but this is not a one-directional empathy deficit in autistic people. Many autistic individuals report high levels of affective empathy (sometimes painfully so) while experiencing specific difficulty with the cognitive empathy dimension in neurotypical social contexts. The EQ, which the original questionnaire was developed to distinguish, measures empathy in a neurotypical cultural context and should be interpreted cautiously for autistic individuals.
About This Test — The EQ Framework
This Empathy Test is inspired by the Empathy Quotient (EQ), a 60-item self-report questionnaire developed by Dr. Simon Baron-Cohen and Dr. Sally Wheelwright at the Autism Research Centre, University of Cambridge (Baron-Cohen & Wheelwright, 2004, Journal of Autism and Developmental Disorders). The EQ was developed as a measure of empathy in adults of normal intelligence and is the most extensively validated and widely used empathy self-report measure in psychological research.
The three-factor structure of the EQ was validated by Lawrence and colleagues (2004, Psychological Medicine), who found that EQ items load onto three factors: Cognitive Empathy (understanding others’ mental states), Emotional Reactivity (affective resonance with others’ emotions), and Social Skills (prosocial behavioral response). This 15-question version covers all three factors across a balanced item set inspired by the full EQ.
The EQ has demonstrated convergent validity with the Reading the Mind in the Eyes Test (Baron-Cohen et al., 2001), the Toronto Alexithymia Scale (Lombardo et al., 2009), and neuroimaging measures of emotion perception (Chakrabarti, Bullmore & Baron-Cohen, 2006).
Answer based on how you generally think, feel, and behave — your habitual patterns across different situations and relationships, not specific moments.
Strongly Disagree = 0 | Disagree = 1 | Neutral = 2 | Agree = 3 | Strongly Agree = 4
Note: Some questions are worded negatively — they ask about difficulty understanding others or not feeling emotional responses. For these questions, agreeing means lower empathy. The scoring adjusts for this automatically.
Total range: 0–60. Higher scores indicate higher empathy. This is a screening tool — it cannot replace a full clinical empathy assessment or address the complexity of your individual empathy profile.
Understanding Your Empathy Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Very Low Empathy | Significant difficulty understanding or sharing others’ emotional experiences across multiple dimensions. Consistent with low empathy profiles associated with alexithymia, psychopathy, or some NPD presentations. |
| 16 – 30 | Below Average Empathy | Empathy is present but limited in one or more dimensions. Some difficulty reading others, lower emotional reactivity, or reduced prosocial motivation compared to the general population. |
| 31 – 45 | Average Empathy | Typical empathy levels — understanding others, some emotional resonance, and prosocial motivation are all reasonably present. Consistent with the general population average. |
| 46 – 60 | High Empathy | Strong empathic capacity across cognitive, affective, and prosocial dimensions. High empathy is a relational strength and also carries specific vulnerability to compassion fatigue in high-demand contexts. |
Can Empathy Be Developed?
Research consistently shows that empathy is not a fixed trait — it is a capacity that responds to deliberate cultivation, motivation, and practice (Zaki, 2019, The War for Kindness, Crown). The key finding: people who believe empathy is a fixed trait that you either have or don’t develop less of it; people who believe empathy is a skill that can be cultivated actually develop more of it over time. The belief itself matters.
Evidence-based practices for developing empathy include: perspective-taking exercises (asking “what is this person thinking and feeling right now?” before responding); active listening practice (focusing entirely on understanding before responding); diverse exposure (reading literature, engaging with experiences different from your own, building genuine relationships across difference); mindfulness (attention training that increases sensitivity to others’ emotional states); and reducing cognitive load in interactions (stress, distraction, and hurry all reduce empathic accuracy).
Frequently Asked Questions
What is an empathy test?
An empathy test is a self-report measure designed to assess an individual’s empathic capacity — their ability to understand others’ mental states (cognitive empathy), feel resonance with others’ emotions (affective empathy), and respond prosocially to both. The most extensively validated empathy self-report instrument is the Empathy Quotient (EQ), developed by Dr. Simon Baron-Cohen and Dr. Sally Wheelwright at the Autism Research Centre, University of Cambridge (2004, Journal of Autism and Developmental Disorders). This test is inspired by that framework, covering all three EQ factors (Lawrence et al., 2004) across 15 questions.
What is the difference between cognitive empathy and emotional empathy?
Cognitive empathy (also called mentalizing or Theory of Mind) is the ability to understand what someone else is thinking and feeling — to accurately model their mental state even when it differs from your own. Emotional (affective) empathy is the ability to feel something in response to what they are feeling — to resonate with their emotional experience rather than simply knowing about it. The two can exist at very different levels in the same person. Narcissistic personality disorder, for example, is characterized by intact or even elevated cognitive empathy combined with significantly reduced affective empathy — the ability to read others accurately coexisting with a lack of felt resonance with their emotional states (Shahri et al., Frontiers in Psychology, 2024). Psychopathy involves a more severe deficit in both dimensions. High-empathy individuals typically have strong performance on both.
Can someone lack empathy entirely?
Complete absence of empathy is exceedingly rare even in clinical populations. More common are significant deficits in one or more dimensions of empathy — reduced cognitive empathy (difficulty reading others), reduced affective empathy (limited emotional resonance), or reduced prosocial motivation (not acting on empathic understanding). Psychopathy involves the most severe empathy deficits and affects approximately 4.5% of the general adult population in subclinical form (Tuvblad et al., systematic review & meta-analysis, Frontiers in Psychiatry, PMC8374040). True absence of empathy is characteristic of full clinical psychopathy and is very rare.
What does low empathy indicate?
Low empathy on this test indicates that one or more of the three empathy dimensions — cognitive understanding, affective resonance, or prosocial motivation — is significantly below average. This can reflect a range of conditions and contexts: narcissistic personality features (reduced affective empathy with intact cognitive); psychopathic traits (reduced across dimensions); alexithymia (difficulty identifying and describing emotions in self and others); compassion fatigue in previously high-empathy individuals; or simply a below-average baseline that, while meaningful for relationships, does not indicate a clinical condition. Low empathy is also significantly more common in males than in females (Baron-Cohen & Wheelwright, 2004).
Is empathy related to emotional intelligence?
Empathy and emotional intelligence (EI/EQ) overlap substantially but are not the same construct. Emotional intelligence, popularized by Dr. Daniel Goleman and grounded in the Salovey-Mayer model, includes: perceiving emotions (in self and others), using emotions to facilitate thought, understanding emotions, and managing emotions. Empathy is a component of emotional intelligence — specifically intersecting with emotion perception and emotion understanding — but emotional intelligence is broader, including self-regulation and emotion management that are not part of the empathy construct as Baron-Cohen defines it. High emotional intelligence typically includes high empathy, but empathy can exist alongside low emotional regulation (as in BPD, where affective empathy is high but emotion management is impaired).
Can empathy be too high?
Yes — and this is an important and often unaddressed clinical question. Very high affective empathy produces specific vulnerabilities: compassion fatigue from chronic emotional resonance with others’ suffering; emotional flooding in high-distress interpersonal situations; boundary difficulties driven by the felt pull toward helping; and the risk of identifying with others’ distress to the point of losing one’s own perspective. High-empathy individuals in caregiving roles, therapy, medicine, or advocacy are particularly vulnerable to these costs. The Burnout Test and Personality Complex Test (particularly the savior complex subscale) are worth completing for high scorers who recognize these patterns.
How does empathy relate to narcissism?
The relationship between empathy and narcissism is more nuanced than “narcissists have no empathy.” Research by Shahri and colleagues (2024, Frontiers in Psychology) demonstrates that narcissistic personality disorder is characterized specifically by intact or even elevated cognitive empathy — the ability to read and understand others’ mental states accurately — combined with significantly reduced affective empathy: “I understand your pain, but I do not feel it.” This pattern means narcissists can be skilled at reading people for strategic purposes while genuinely experiencing little resonance with their distress. Lack of empathy correlates with grandiosity in approximately 85% of NPD cases (Gitnux, 2026). The NPD Test and Covert Narcissism Test are worth completing alongside this one.
Related Tests
- Narcissistic Personality Disorder Test — NPD is characterized by reduced affective empathy with intact cognitive empathy; the most clinically significant empathy profile difference from the general population
- Covert Narcissism Test — covert narcissism involves the same empathy deficit pattern through a different personality presentation
- Dark Triad Test — all three Dark Triad traits (narcissism, Machiavellianism, psychopathy) are associated with reduced affective empathy; the Dark Triad profile is the most research-linked personality configuration for low empathy
- Psychopath Test (PCL-R) — psychopathy involves the most severe empathy deficit documented in personality research; callousness and lack of remorse are core features
- Antisocial Personality Disorder Test — ASPD includes persistent disregard for others’ rights; reduced empathy is a central feature
- Borderline Personality Disorder Test — BPD involves high affective empathy that produces emotional flooding rather than empathy deficit; important distinction from NPD/psychopathy profiles
- Burnout Test — compassion fatigue through depletion of high empathy is a documented burnout pathway; essential for high scorers in caregiving roles
- Personality Complex Test — the savior complex subscale assesses whether high empathy has become organized into a compulsive helping pattern
- Social Anxiety Test — social anxiety can produce behaviors that resemble low empathy (reduced social curiosity, limited engagement) through anxiety rather than empathy deficit
- Emotional Availability Test — emotional availability (the capacity to be emotionally present and responsive in relationships) overlaps significantly with prosocial empathy dimension
References
- Baron-Cohen, S., & Wheelwright, S. (2004). The Empathy Quotient: An investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. Journal of Autism and Developmental Disorders, 34(2), 163–175. [EQ development; sex differences; AS group norms] autismresearchcentre.com
- Lawrence, E.J., Shaw, P., Baker, D., Baron-Cohen, S., & David, A.S. (2004). Measuring empathy: Reliability and validity of the Empathy Quotient. Psychological Medicine, 34(5), 911–924. [Three-factor structure: cognitive empathy, emotional reactivity, social skills] researchgate.net
- Zaki, J., & Ochsner, K. (2012). The neuroscience of empathy: Progress, pitfalls and promise. Nature Neuroscience, 15(5), 675–680. [Three facets: mentalizing, experience sharing, prosocial concern] doi.org/10.1038/nn.3085
- Shahri, F., Zabihzadeh, A., Taqipanahi, A., et al. (2024). I understand your pain but I do not feel it: lower affective empathy in response to others’ social pain in narcissism. Frontiers in Psychology, 15, 1350133. [Cognitive intact; affective reduced in NPD] doi.org/10.3389/fpsyg.2024.1350133
- Zaki, J. (2019). The War for Kindness: Building Empathy in a Fractured World. Crown. [Empathy as trainable skill; mindset matters; mindfulness and perspective-taking]
- Tuvblad, C., et al. (2021). Prevalence of psychopathy in the general adult population: A systematic review and meta-analysis. Frontiers in Psychiatry. [4.5% general population prevalence] pmc.ncbi.nlm.nih.gov
- Brown, B. (2010). The power of vulnerability. TEDxHouston. [Empathy vs sympathy distinction; connection through vulnerability] ted.com
- Milton, D. (2012). On the ontological status of autism: the ‘double empathy problem’. Disability & Society, 27(6), 883–887. [Double empathy problem; autism-empathy nuance] doi.org/10.1080/09687599.2012.710008
- Wikipedia. (2025). Empathy quotient. en.wikipedia.org