
The four Cluster B personality disorders — Borderline (BPD), Narcissistic (NPD), Histrionic (HPD), and Antisocial (ASPD) — are grouped together in the DSM-5-TR’s “dramatic, emotional, or erratic” cluster for a reason. They share a superficial family resemblance: emotional intensity, difficulty maintaining stable relationships, impulsive behavior, and the capacity to cause significant distress for both the person who has them and those around them. But beneath that shared surface, each disorder has a distinct structure, core dynamic, and treatment approach.
Understanding which Cluster B pattern is most prominent — whether in yourself or in someone significant in your life — is clinically important because the four disorders can present similarly on the surface while requiring quite different responses. The fear-of-abandonment-driven dysregulation of BPD is not the entitlement-driven exploitation of NPD, which is not the attention-seeking theatricality of HPD, which is not the callous rule-violation of ASPD — even when they can all produce similar chaos in the relationships around them.
This free Cluster B Personality Disorder test screens for the most clinically significant features of all four disorders using DSM-5-TR criteria (APA, 2022). 15 questions. Instant results identifying which Cluster B pattern is most prominent in your profile.
If you are experiencing thoughts of self-harm or suicide, please reach out now.
Call or text 988 (Suicide & Crisis Lifeline, US, 24/7) | Text HOME to 741741 (Crisis Text Line)
What Are Cluster B Personality Disorders?
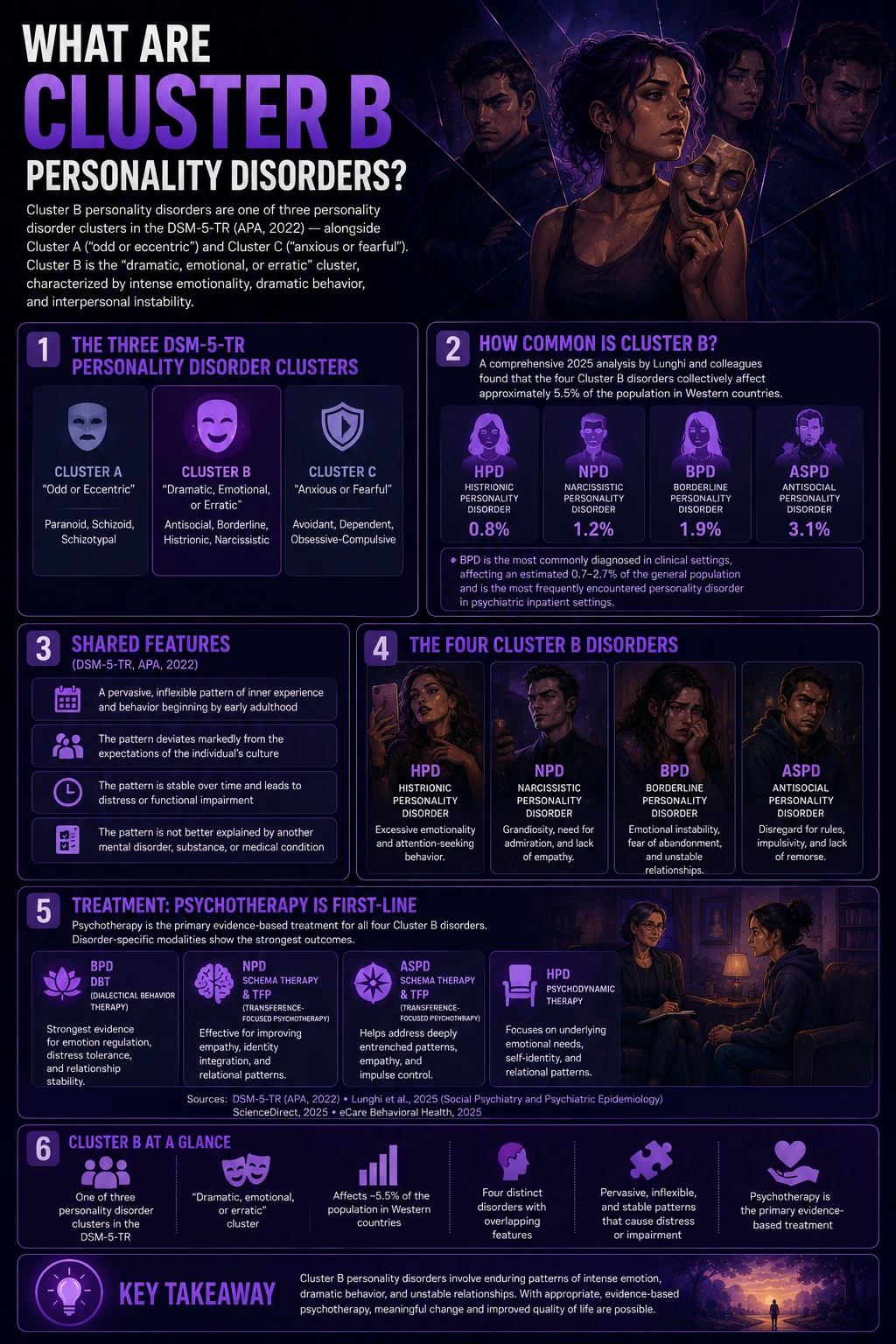
Cluster B personality disorders are one of three personality disorder clusters in the DSM-5-TR (APA, 2022) — alongside Cluster A (“odd or eccentric”) and Cluster C (“anxious or fearful”). The DSM-5-TR classifies Cluster B as the “dramatic, emotional, or erratic” cluster, characterized by intense emotionality, dramatic behavior, and interpersonal instability.
The four Cluster B disorders collectively affect approximately 5.5% of the population in Western countries, according to a comprehensive 2025 analysis by Lunghi and colleagues (Social Psychiatry and Psychiatric Epidemiology, 2025). Subtype prevalence estimates: HPD 0.8%, NPD 1.2%, BPD 1.9%, and ASPD 3.1% (Lunghi et al., 2025). BPD is the most commonly diagnosed in clinical settings, affecting an estimated 0.7–2.7% of the general population and representing the most frequently encountered personality disorder in psychiatric inpatient settings (ScienceDirect, 2025; eCare Behavioral Health, 2025).
All four disorders share the following features per DSM-5-TR (APA, 2022):
— A pervasive, inflexible pattern of inner experience and behavior beginning by early adulthood
— The pattern deviates markedly from the expectations of the individual’s culture
— The pattern is stable over time and leads to distress or functional impairment
— The pattern is not better explained by another mental disorder, substance, or medical condition
Psychotherapy is the primary evidence-based treatment for all four Cluster B disorders, with disorder-specific modalities showing the strongest outcomes: DBT for BPD, Schema Therapy and TFP for NPD and ASPD, and psychodynamic therapy for HPD (Lunghi et al., 2025; APA, 2022).
The Four Cluster B Disorders — What Makes Each One Distinct
Borderline Personality Disorder (BPD) — DSM-5-TR 301.83 (F60.3)
The core of BPD is fear of abandonment and identity instability. The emotional dysregulation, impulsivity, self-harm, splitting, and chronic emptiness of BPD are all organized around the terror of being left and the absence of a stable self. BPD is the most common Cluster B disorder in clinical settings and has the most extensively evidence-based treatment in DBT (Dialectical Behavior Therapy), developed by Dr. Marsha Linehan. Requires ≥5 of 9 DSM-5-TR criteria. Prevalence: 0.7–2.7%; more common in females in clinical samples, roughly equal in community samples.
Narcissistic Personality Disorder (NPD) — DSM-5-TR 301.81 (F60.81)
The core of NPD is grandiosity and need for admiration — a self-concept that is both inflated and fragile, requiring continuous external validation to sustain. The entitlement, exploitation, empathy deficit, and arrogance of NPD are organized around the protection and maintenance of the grandiose self-image. Requires ≥5 of 9 DSM-5-TR criteria. Prevalence: 1.2% (Lunghi et al., 2025); diagnosed 3× more often in males (APA, 2022). The most central criterion: need for admiration (Gori & Topino, Clinical Psychology & Psychotherapy, 2025, N=376).
Histrionic Personality Disorder (HPD) — DSM-5-TR 301.50 (F60.4)
The core of HPD is excessive emotionality and attention-seeking. The seductiveness, theatricality, impressionistic speech, shallow emotional expression, and systematic overestimation of relationship intimacy of HPD are all organized around the need to be the center of attention. Requires ≥5 of 8 DSM-5-TR criteria. Prevalence: 0.8% (Lunghi et al., 2025); the least prevalent of the four Cluster B disorders. Diagnosed approximately 4× more often in females, though diagnostic bias is documented (APA, 2022).
Antisocial Personality Disorder (ASPD) — DSM-5-TR 301.7 (F60.2)
The core of ASPD is a persistent disregard for and violation of others’ rights — a pervasive pattern that includes deceitfulness, impulsivity, aggressiveness, reckless disregard for safety, irresponsibility, and a lack of remorse. The most prevalent of the four Cluster B disorders at 3.1% (Lunghi et al., 2025), ASPD is 3× more common in males. It requires a history of conduct disorder before age 15 (DSM-5-TR Criterion B) and cannot be diagnosed before age 18. It is the Cluster B disorder most closely related to the forensic construct of psychopathy.
Signs You Might Have a Cluster B Personality Disorder
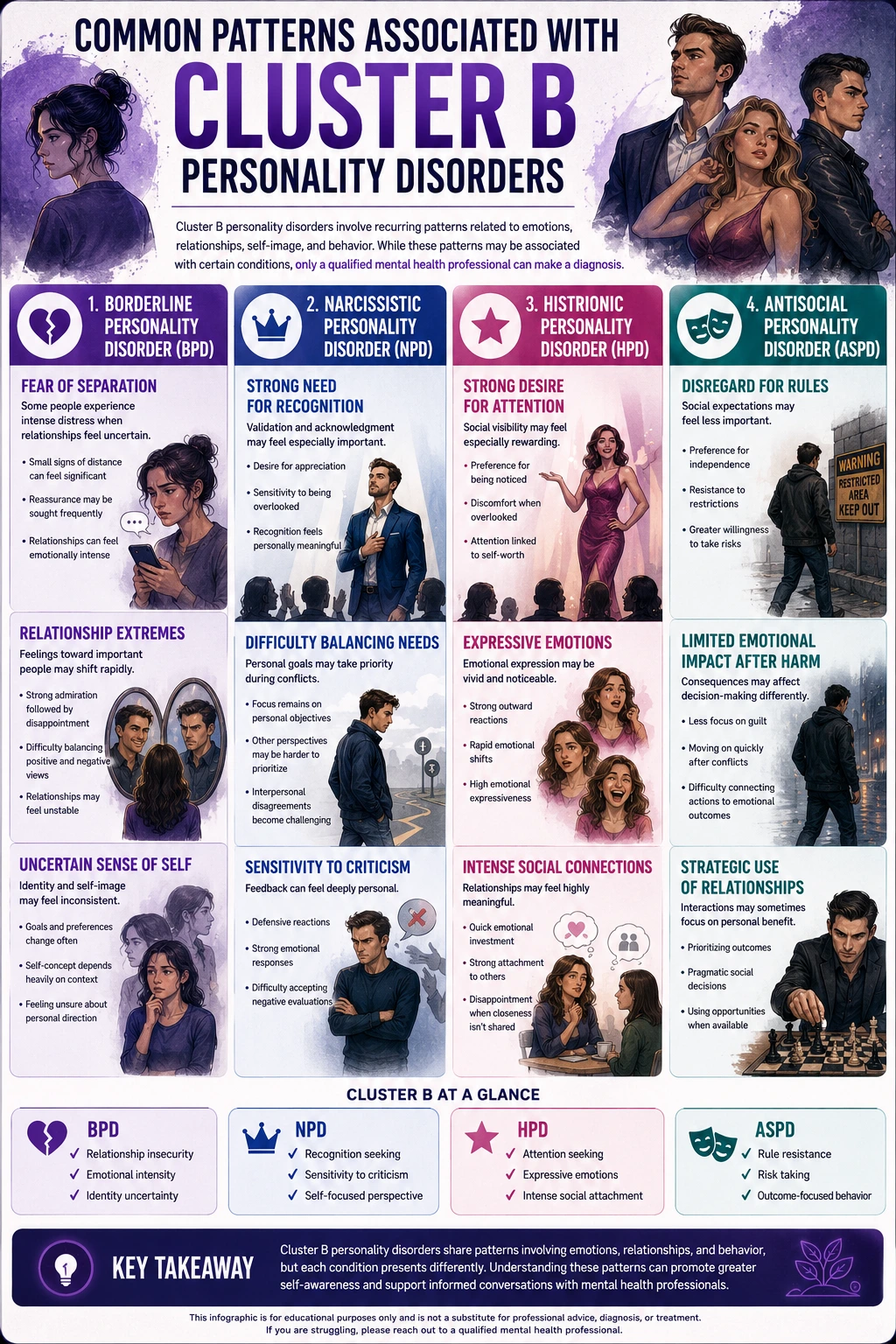
The Cluster B disorders share a family resemblance but have distinct experiential signatures. These signs are organized by the pattern most associated with each disorder — recognize which resonates most consistently.
Signs most consistent with BPD:
The fear of being left is constant — and activates before there’s clear evidence it’s happening. A slight distance, a delayed reply, a shift in someone’s tone — and the abandonment panic is immediate, physical, and complete. The response — clinging, rage, desperate action — is disproportionate to any actual signal.
The people in your life are either wonderful or terrible — and the same person can be both within the same day. Splitting — the alternation between idealization and devaluation — produces a relational world of extremes. Ambivalence (holding love and disappointment simultaneously about the same person) is very difficult to sustain.
You are not sure who you are when you’re not in a relationship — your sense of self shifts significantly depending on who you’re with. The identity disturbance of BPD is not ordinary self-consciousness; it is a deeper uncertainty about values, wants, and core identity that depends on the relational context to feel stable.
Signs most consistent with NPD:
You expect recognition and deference — and feel genuinely injured when you don’t receive them. Not disappointment but something more like indignation: something owed to you has been withheld. The recognition feels like a right, not a preference.
You find it genuinely difficult to care about others’ feelings when they conflict with what you want. The empathy deficit of NPD is not cruelty — it is the structural inability to consistently let others’ emotional states outweigh your own needs and goals when they conflict. The empathy can be demonstrated situationally; it fails when it costs something.
Criticism activates anger or contempt rather than reflection. Negative evaluation doesn’t land as information to update your self-model — it lands as a threat to be repelled. The response is typically dismissal of the critic, counterattack, or cold contempt rather than genuine consideration.
Signs most consistent with HPD:
Being unnoticed in a social situation feels genuinely intolerable — not just uncomfortable. The discomfort when not the center of attention that DSM-5-TR Criterion 1 describes is qualitatively different from ordinary preference for recognition. It is a structural inability to tolerate not being the focal point.
Your emotional responses are rapid, intense, and sometimes feel theatrical even to you. The rapidly shifting, shallow emotional expression of HPD (Criterion 3) — emotions that are vivid in the moment and resolve quickly in ways others find inconsistent — is recognizable from the inside as well as from the outside.
You experience relationships as significantly more intimate and meaningful than the other person seems to. The systematic overestimation of relationship intimacy (Criterion 8) produces a recurring pattern of investing deeply in connections that others experience as more casual — and being confused and hurt when they don’t reciprocate the intensity.
Signs most consistent with ASPD:
Rules, laws, and social norms feel like constraints that apply to other people — not to you. The pervasive disregard for social rules that defines ASPD is not primarily experienced as rebellion; it is a fundamental orientation in which the rules simply feel less binding than they apparently do for most people.
You feel very little remorse when your actions harm others — or the remorse that arrives is brief and doesn’t reliably change your behavior. The lack of remorse that characterizes ASPD (Criterion 7) is one of its most diagnostically specific features — distinguishing it from impulsive behavior driven by shame or guilt that constrains future action.
You have a history of deceiving, manipulating, or exploiting others for personal gain across multiple relationships and contexts. The pervasive deceitfulness of ASPD (Criterion 2) extends across relationships and contexts, distinguishing it from situational dishonesty or the strategic deception of Machiavellianism.
How the Four Cluster B Disorders Relate and Differ
| Feature | BPD | NPD | HPD | ASPD |
|---|---|---|---|---|
| Core dynamic | Fear of abandonment + unstable identity | Grandiosity + need for admiration | Excessive emotionality + attention-seeking | Persistent disregard for others’ rights |
| Emotional style | Intense, reactive, dysregulated — driven by interpersonal triggers | Controlled; rage when ego threatened; flat between challenges | Rapid, shallow, theatrical — expressed for audience effect | Flat or callous; anger as a tool; low guilt and remorse |
| Relationship pattern | Intense splitting; frantic abandonment avoidance; idealization-devaluation | Exploitation; idealize those who validate; devalue those who don’t | Seductive; overestimates intimacy; focused on exciting new connections | Exploitative without guilt; relationships as means to ends; serial deception |
| Self-harm / suicide risk | High — Criterion 5; ~8–10% complete suicide; self-harm as emotion regulation | Lower but present; narcissistic injury can produce suicidality | Moderate — suicidal gestures can be attention-seeking but carry real risk | Elevated due to impulsivity; accidental harm and reckless behavior |
| Prevalence | 1.9% (0.7–2.7%) | 1.2% | 0.8% | 3.1% |
| Sex distribution | Female > male in clinical; roughly equal in community | 3× more diagnosed in males | 4× more diagnosed in females (diagnostic bias documented) | 3× more prevalent in males |
| DSM code | 301.83 (F60.3) | 301.81 (F60.81) | 301.50 (F60.4) | 301.7 (F60.2) |
| Primary treatment | DBT (gold standard); MBT; TFP | Schema Therapy; TFP | Psychodynamic therapy; CBT; Schema Therapy | CBT; contingency management; limited evidence base |
| PsyMed test | BPD Test | NPD Test | HPD Test | ASPD Test |
How This Cluster B Personality Disorder Test Works
This Cluster B test screens for the most clinically significant features of all four DSM-5-TR Cluster B disorders across 15 questions — 4 items covering BPD features, 4 covering NPD features, 4 covering ASPD features, and 3 covering HPD features, weighted by clinical prevalence and discriminating power. The questions target the core features that most reliably distinguish each disorder.
Answer based on your consistent pattern over the past 12 months across different situations and relationships — not isolated incidents or your best or worst periods. The test can also be answered about someone in your life by responding based on how they typically behave.
- Never = 0
- Rarely = 1
- Sometimes = 2
- Often = 3
- Always = 4
Total range: 0–60. Your result will identify your overall Cluster B indicator level and highlight which Cluster B pattern scored highest based on your answers. Only a qualified mental health professional can diagnose any personality disorder.
Understanding Your Cluster B Personality Disorder Test Score
| Score Range | Category | What It Suggests |
|---|---|---|
| 0 – 15 | Low — Few Cluster B Indicators | Few significant Cluster B personality disorder patterns present. Normal emotional intensity and relationship challenges may be present without a pattern consistent with Cluster B disorders. |
| 16 – 30 | Mild — Some Cluster B Patterns | Some Cluster B-related features present across one or more disorder domains. May reflect subclinical traits or early-stage patterns. Note which disorder’s questions scored highest for the most relevant picture. |
| 31 – 45 | Moderate — Significant Cluster B Pattern | Significant Cluster B features across multiple criterion domains. Consistent with a Cluster B personality disorder presentation. Professional evaluation is recommended. |
| 46 – 60 | High — Strong Cluster B Indicators | Pervasive Cluster B pattern across most domains. Strongly consistent with a Cluster B personality disorder diagnosis. Professional evaluation and specialized treatment are urgently recommended. |
What Causes Cluster B Personality Disorders?
No single cause explains the Cluster B disorders — they share a multifactorial etiology involving genetic vulnerability, developmental experience, and neurobiological factors, with the specific weighting differing by disorder.
Genetic factors. All four Cluster B disorders show significant heritability in twin studies — BPD at 40–60%, NPD and ASPD at similar ranges. The genetic contribution likely reflects temperamental vulnerabilities — emotional reactivity in BPD and HPD, antagonism in NPD, impulsivity and callousness in ASPD — that interact with developmental experience to produce the full disorder.
Developmental and attachment factors. Adverse Childhood Experiences (ACEs) — including abuse, neglect, and attachment disruption — are significantly associated with all Cluster B disorders. A 2024 prospective longitudinal study by Broekhof and colleagues (Journal of Personality Disorders, 2024(38)) found that ACEs are significantly associated with personality disorder development. BPD shows the strongest trauma connection; ASPD frequently involves childhood conduct disorder preceding adult presentation.
Neurobiological factors. Each Cluster B disorder has documented neurobiological correlates: BPD involves amygdala hyperreactivity and prefrontal cortex regulatory deficits; NPD shows structural differences in insular cortex regions associated with empathy processing; ASPD involves reduced amygdala response to fear stimuli and prefrontal dysfunction; HPD is less studied neurobiologically but is associated with elevated reward sensitivity.
Comorbidities. The four Cluster B disorders co-occur with each other and with Axis I conditions at high rates. Outpatients with depressive disorders are 3.72 times more likely to have a Cluster B personality disorder (eCare Behavioral Health, 2025). PTSD and Cluster B disorders frequently co-occur, particularly BPD and NPD. ADHD shares impulsivity and emotional dysregulation with BPD and ASPD. Major depressive disorder is the most common comorbid Axis I condition across all four disorders.
Frequently Asked Questions
What are Cluster B personality disorders?
Cluster B personality disorders are the four DSM-5-TR disorders grouped under the “dramatic, emotional, or erratic” classification: Borderline Personality Disorder (BPD, 301.83), Narcissistic Personality Disorder (NPD, 301.81), Histrionic Personality Disorder (HPD, 301.50), and Antisocial Personality Disorder (ASPD, 301.7). They collectively affect approximately 5.5% of the population in Western countries (Lunghi et al., Social Psychiatry and Psychiatric Epidemiology, 2025), with subtype prevalence: HPD 0.8%, NPD 1.2%, BPD 1.9%, ASPD 3.1%. All four share the DSM criteria for personality disorders: pervasive, inflexible patterns beginning in early adulthood that deviate from cultural expectations and cause distress or impairment.
Can you have more than one Cluster B disorder?
Yes — co-occurring Cluster B disorders are well-documented in the research literature. BPD and NPD share features of splitting and idealization-devaluation and frequently co-occur. BPD and ASPD share impulsivity and emotional dysregulation and can co-occur. HPD and NPD both involve attention-seeking and share some surface features. Research documents that multiple personality disorder diagnoses are common in clinical populations, and that the four Cluster B disorders are not mutually exclusive. This is one reason the individual disorder tests — the BPD Test, NPD Test, HPD Test, and ASPD Test — provide a more granular picture than this combined screening.
How are Cluster B disorders different from Cluster A and Cluster C?
The three clusters describe distinct personality disorder patterns. Cluster A (“odd or eccentric”) includes Paranoid, Schizoid, and Schizotypal Personality Disorders — characterized by unusual thinking, social isolation, and eccentric behavior. Cluster B (“dramatic, emotional, or erratic”) includes the four disorders covered in this test — characterized by emotional intensity, impulsivity, and interpersonal drama. Cluster C (“anxious or fearful”) includes Avoidant, Dependent, and Obsessive-Compulsive Personality Disorders — characterized by anxiety, fear, and inhibition. The clusters are descriptive groupings rather than etiological categories — disorders within each cluster share surface similarities but have distinct causes and treatments.
Which Cluster B disorder is most common?
ASPD is the most prevalent Cluster B disorder at approximately 3.1% of the Western population (Lunghi et al., 2025), though it is significantly more prevalent in males (3× more common) and in criminal justice settings. BPD is the most commonly diagnosed Cluster B disorder in clinical and psychiatric settings, affecting 0.7–2.7% of the general population and representing a disproportionate share of psychiatric inpatient admissions (ScienceDirect, 2025; eCare, 2025). NPD affects approximately 1.2% and HPD approximately 0.8% (Lunghi et al., 2025).
Are Cluster B personality disorders treatable?
Yes — the view that personality disorders are untreatable has been comprehensively overturned. All four Cluster B disorders respond to appropriate, specialized treatment: BPD has the most robust evidence base with DBT (Dialectical Behavior Therapy) by Dr. Marsha Linehan producing significant improvements in suicidality, self-harm, and emotional dysregulation; NPD responds to Schema Therapy and Transference-Focused Psychotherapy (TFP); HPD responds to psychodynamic approaches and CBT; ASPD has the most limited evidence base but structured CBT and contingency management produce some improvement. Psychotherapy is the primary treatment for all four, with medication adjunctive rather than primary (Lunghi et al., 2025).
What distinguishes Cluster B personality disorders from normal emotional intensity?
The distinction lies in three features the DSM-5-TR requires for any personality disorder diagnosis: pervasiveness (the pattern appears across many different situations and relationships, not just specific contexts), stability (the pattern has been consistent since early adulthood, not reactive to recent circumstances), and impairment (the pattern causes clinically significant distress or functional impairment in important life domains). Everyone experiences intense emotions, relationship difficulties, self-centered moments, and impulsive behavior occasionally — these are normal human experiences. What distinguishes Cluster B personality disorders is the inflexibility, the pervasiveness across contexts, the consistency over time, and the degree of impairment they cause. A single dramatic episode, a difficult period, or a particularly stressful relationship does not constitute a personality disorder. It is the enduring pattern — present across different relationships, different contexts, and different life periods — that meets the clinical threshold (APA, 2022; Lunghi et al., 2025).
How is this test different from the individual Cluster B disorder tests?
This test is a broad screening across all four Cluster B disorders simultaneously — 15 questions covering the most clinically significant features of each disorder in a combined format. It is designed to identify which Cluster B pattern is most prominent and to direct you to the appropriate individual test for fuller assessment. The individual tests — BPD Test (18 questions covering all 9 criteria), NPD Test (15 questions covering all 9 criteria), HPD Test (15 questions covering all 8 criteria), and ASPD Test — provide significantly more granular clinical information for each specific disorder.
Related Tests
- Borderline Personality Disorder Test — full 18-question BPD screening covering all 9 DSM-5-TR criteria; gold-standard reference for the most common Cluster B clinical presentation
- Narcissistic Personality Disorder Test — full NPD screening covering all 9 criteria, including both grandiose and covert presentations
- Histrionic Personality Disorder Test — full HPD screening covering all 8 DSM-5-TR criteria
- Antisocial Personality Disorder Test — full ASPD screening; the most prevalent Cluster B disorder
- Covert Narcissism Test — vulnerable narcissism assessed via the MCNS framework; captures the NPD subtype most frequently missed by standard assessments
- Dark Triad Test — measures subclinical narcissism, Machiavellianism, and psychopathy across 15 questions; overlaps with NPD and ASPD dimensions
- Psychopath Test (PCL-R) — clinical psychopathy assessment; ASPD and psychopathy overlap significantly but are not identical
- PTSD Test — PTSD and BPD frequently co-occur and are among the most important differentials; trauma assessment is essential alongside Cluster B screening
- Bipolar Test — bipolar disorder is among the most commonly confused conditions with BPD; important differential for emotional dysregulation
- Empathy Test — reduced empathy is a shared feature of NPD, ASPD, and psychopathy; complementary assessment
- Full Personality Disorder Test Hub — all ten DSM-5-TR personality disorder types across Clusters A, B, and C
References
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Cluster B Personality Disorders (pp. 748–771). psychiatry.org
- Lunghi, C., Cailhol, L., Massamba, V., et al. (2025). Cluster B personality disorders and psychotropic medications: a focused analysis of trends and patterns across sex and age groups. Social Psychiatry and Psychiatric Epidemiology, 60, 1499–1509. [5.5% Western prevalence; subtypes: HPD 0.8%, NPD 1.2%, BPD 1.9%, ASPD 3.1%; psychotherapy primary] link.springer.com
- Leichsenring, F., Fonagy, P., Heim, N., et al. (2024). Borderline personality disorder: a comprehensive review of diagnosis and clinical presentation, etiology, treatment, and current controversies. World Psychiatry, 23(1), 4–25. [DBT; personality disorders treatable] pmc.ncbi.nlm.nih.gov
- ScienceDirect. (2025). Understanding borderline personality disorder: Clinical features, neurobiological insights, and therapeutic strategies. [BPD 0.7–2.7%; sex differences; DBT gold standard] sciencedirect.com
- Broekhof, R., Nordahl, H.M., Eikenæs, I.U., & Selvik, S.G. (2024). Adverse Childhood Experiences Are Associated With Personality Disorder: A Prospective, Longitudinal Study. Journal of Personality Disorders, 38(1), 19–33. pubmed.ncbi.nlm.nih.gov
- Gori, A., & Topino, E. (2025). DSM-5-TR Criteria and Domains for Narcissistic Personality Disorder: Evidence From Network Analysis. Clinical Psychology & Psychotherapy, 32(6), e70179. [Need for admiration = most central NPD node; N=376] doi.org
- eCare Behavioral Health Institute. (2025). 20 Personality Disorder Statistics for 2025. [3.72× Cluster B in depression outpatients; BPD 28.5% inpatient] ecarebehavioralinstitute.com
- Cleveland Clinic. (2025). Cluster B Personality Disorders: What They Are and Traits. my.clevelandclinic.org
- Wikipedia. (2025). Cluster B personality disorders. en.wikipedia.org